Download
1 / 41
410 likes | 599 Vues
This presentation covers recent updates on thyroid disorders, focusing on the nuances of interpreting thyroid function tests like TSH and Free T4 in clinical practice. It discusses cases of atrial fibrillation, fatigue, and enlarged thyroids, emphasizing the importance of both tests for accurate diagnosis. The presentation explores the implications of subclinical and overt hyperthyroidism and hypothyroidism, detailing testing strategies, associated risks, and treatment options such as anti-thyroid drugs and radioiodine. Clinical recommendations for managing these conditions are also highlighted.

E N D
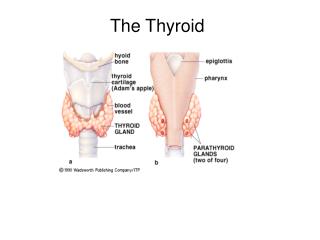
Update on the Thyroid Douglas C. Bauer, MD UCSF Division of General Internal Medicine No Disclosures
Cases • 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 • 79 yr old man with 1 yr of fatigue and lassitude and no findings except TSH=9.0, anti-TPO positive • 45 yr old women, enlarged thyroid with dominant nodule since 1999, FNA benign. On T4 suppession ever since, TSH=0.1
Thyroid Tests: sTSH • Very sensitive to circulating thyroid hormone levels • Excellent correlation with TRH stimulation (sTSH < 0.1) • Requires intact pituitary-hypothalamic axis;4-6 weeks to equilibrate • Falsely low: severe illness, corticosteriods, dopamine • Normal range 0.5-4.8 mU/L; $58
Thyroid Tests: Free Thyroxine • Measures unbound hormone • Replacing “index” assays • Gold standard: Equilibrium dialysis • Other immunoassays: Improving • Normal range, 9-24 pmol/L; $64
Are Both sTSH and Free T4 Necessary? • American Thyroid Association: Yes • Others recommend sTSH first • UCSF outpatient data • Results when both tests ordered on the same specimen (N=3143) • Each test classified as low, normal or high
Diagnostic Redundancy of sTSH and Free T4 sTSH (mU/L)< 0.5 0.5 - 5.5 > 5.5 < 9 4 16 49 9 - 24 536 2024 309 > 24 174 30 1 Free T4 (pmol/L)
Subclinical Thyroid Disease • Subclinical hypothyroidism“Abnormally high sensitive TSH and normal thyroid hormone levels” • Subclinical hyperthyroidism“Abnormally low sensitive TSH and normal thyroid hormone levels”
Suggested Testing Strategy • If sTSH is normal, STOP • If sTSH is low, measure T4, consider T3 • If sTSH is high, measure T4, consider TPO antibodies
Thyroid Antibodies • Anti-thyroperoxidase, TPO (titer<100, $78) • Similar to “anti-microsomal” • Most sensitive thyroid autoantibody • Specificity a problem • TSH receptor antibody (absent, $112) • Causes Grave’s disease • Rarely found in normal individuals
Thyroid Scans • Technetium 99 ($450) • Low radiation, quick • Useful for nodules in some circumstances • Useful to determine cause of hyperthyroidism • A. High uptake: Grave’s, toxic nodule • B. Low uptake: thyroiditis, thyroxine use
Hyperthyroidism: Epidemiology • Etiology: • Iatrogenic • A. Over replacement (30-50% given rx) • B. Suppression of CA, goiters, and nodules • Autoimmune (Grave’s disease): thyroid stimulating autoantibodies • Autonomous nodule(s). Occasionally T3 • TSH secreting tumors
Hyperthyroidism: Prevalence • Population based prevalence of suppressed TSH:AuthoragemenwomenBagchi (1990) >55 1.8% 2.7%Falkenberg (1991) >60 1.9%Parle (1991) >60 5.5 6.3%Bauer (1993) >55 5.8%
Hyperthyroidism in the Elderly • Weight loss, palpitations, and nervousness less common • Tachycardia, exophthalmos, tremor less common • Atrial fibrillation more common • 8-10% are completely asymptomatic
Subclinical Hyperthyroidism: Cardiac Effects • Systolic time intervals shortened • Clinical significance uncertain • Reduced exercise tolerance • Increased incidence of atrial fibrillation Swain, 1994 Prospective cohort, N = 2000 RR = 3.1 (1.7, 5.5) if sTSH < 0.1
Subclinical Hyperthyroidism: Skeletal Effects • Florid hyperthyroidism causes fractures • Effect on BMD, bone loss controversial • Increased fracture risk (Bauer, 2001)- Prospective study, 9407 older women- TSH < 0.1 vs. normal- Hip fracture: RR = 3.6 (1.0, 12. 9)- Vertebral fracture: RR = 4.5 (1.3, 15.6) • Effect of accelerated bone turnover?
Subclinical Hyperthyroidism: Natural History • Exogenous: Well established • Endogenous: Little longitudinal data Parle, 1991 50 untreated individuals >60 1 developed overt hyperthyroidism After 1 year, sTSH normal in half!
Who Should Be Treated? • Exogenous (iatrogenic) • Dose reduction unless contraindicated • Endogenous (subclinical) • Follow if uncomplicated • Consider treatment if atrial fibrillation or osteoporosis present • Endogenous (overt) • Rule out thyroiditis • Tx everyone else with beta blocker and...
Hyperthyroidism: Treatment • Anti-thyroid drugs (PTU and methimazole) • Remission: 30-50% after 12-18 mo • Side effects: rash, fever, arthritis, agranulocytosis (all rare) • Radioiodine • Best treatment for hot nodules • Remission: everyone • Side effects: transient thyroiditis (rare), hypothyroid (50%), worsening exophthalmous
Radioiodine and Mortality • Franklyn, 1998- 7209 hyperthyroid pts, 15 yr follow-up- All cause mortality: 13% higher than age and sex matched populations- CV deaths increased, but not cancer • Mechanism unknown, clear dose-response • Unable to adjust for other potential confounders
Hypothyroidism: Epidemiology • Etiology • Autoimmune (Hashimoto’s) • Iodine deficiency • Iatrogenic A. Radioiodine/ surgery B. Drugs (lithium, amiodarone) • Pituitary/ hypothalamic disease
Hypothyroidism: Prevalence • Population based prevalence of elevated TSH: Author age men women Tunbridge(1977) >65 6.0% 10.9% Bagchi(1990) >55 1.8% 2.7% Parle(1991) >60 2.9% 11.6%Bauer(1993) >55 5.4%
Overt Hypothyroidism in the Elderly • “Classic” features often missing • Neuropsychiatric complaints common: depression, weakness, memory loss • Other clues: hypercholesterolemia, elevated CK, pleural effusion
Subclinical Hypothyroidism: CV Outcomes • Observational studies • Total cholesterol unchanged, but higher LDL and lower HDL? • What about atherosclerosis? • Rotterdam population-based study (Hak, 2000) • 1149 women, mean age 70 • Subclinical hypo (TSH > 4, nl T4) in 10.8% • Aortic atherosclerosis RR = 1.7 (1.1, 2.6) • History of MI RR = 2.3 (1.3, 4.0)
Meta Analysis of Subclinical Hypothyroidism and CHD Summary OR 1.65 (1.28-2.12) P for heterogeneity: 0.12
Subclinical Hypothyroidism: Other Outcomes • Observational studies of neuropsychiatric symptoms • Conflicting evidence • Four small double blinded trials, sTSH > 5-7 • Randomized to thyroxine or placebo • No significant change in weight, lipids, other laboratory values • Psychometric testing: Treated felt better and had better memory scores
Subclinical Hypothyroidism: Natural History • Many good studies • Spontaneous resolution infrequent • Antibodies strongly influence outcome • If TPO positive, overt hypothyroidism 5%/yr
Hypothyroidism: Treatment • Replace with thyroxine (T4) • T3 + T4 benefit unproven • Typical replacement dose 1.6 mcg/kg • Elderly or CAD: start low (0.025-0.05 mg/d), gradually increase dose • Maintain TSH within the normal range • Wait 6 weeks after dose change • Monitor yearly (noncompliance, reduced T4 clearance)
What About Treatment of Symptomatic but Euthyroid Patients? Forget It. • Symptoms of hypothyroidism common • Real but not detected by usual tests? • Double blind RCT (Pollock, 2001) • 25 “symptomatic”, 18 “controls” • All euthyroid • 3 mo of T4 (0.1/d) or placebo, cross-over • TSH fell with T4 tx but no difference in cognitive or psychological function
Thyroid Nodules: Epidemiology and Evaluation • Nodules are common (and cancer is rare) • 90% women over age 60 have one or more thyroid nodules at autopsy • Risk factors for cancer: neck irritation, FH • Evaluation: FNA first • 75% benign, 20% suspicious, 5% malignant • Best centers: false negative 2% false positive 1%
Thyroid Nodules: Treatment • Cancer- Histology is important (papillary best)- Surgery and 131I ablation - Suppression with T4? TSH = 0.1-0.4 • Benign nodules- Many shrink spontaneously- Meta analysis of T4 suppression Smaller: 26% vs. 12% (NNT=7) Larger: 8% vs. 17% (NNT=11)- T4 doesn’t prevent new nodules
Screening Cost-effectiveness • Danese and Sawin, 1995 • Cost-utility analysis, sTSH-based screening • Modeled progression, symptoms and CAD • Screening every 5 year from 35-65: $9,223 per QALY in women $22,595 per QALY in men • Sensitivity analysis: cost of TSH key ($25)
Screening for Subclinical Thyroid Disease • US Preventive Task Force, 1996“Routine screening is not recommended. Insufficient evidence for high risk patients, including elderly.” • ACP, 1998“It is reasonable to screen women older than 50 years of age for unsuspected but symptomatic thyroid disease.”
Screening Cost-effectiveness • Effects on HDL, fractures not included. Cost of testing overestimated ($3/TSH) • Published analyses underestimatecost-effectiveness • Other unresolved issues: • Age to start screening? • Optimal frequency?
Summary Take Home Points • sTSH is best test • Subclinical thyroid disease is common, associated with morbidity, and treatable • Low threshold to treat subclinical hypo • Treatment threshold for subclinical hyper less certain • Screening with sTSH is cost-effective
Cases • 68 yr old female with new atrial fibrillation and no other findings except TSH=0.04, normal free T4 • 79 yr old man with 1 yr of fatigue and lassitude and no findings except TSH=9.0, anti-TPO positive • 45 yr old women, enlarged thyroid with dominant nodule since 1999, FNA benign. On T4 suppession ever since, TSH=0.1