Download
1 / 20
270 likes | 880 Vues
Adverse Reactions to Contrast Media. Ri 陳達慶. Articles. Acute serious and fatal reactions to contrast media: our current understanding S K Morcos, FRCS, FRCR British Journal of Radiology ( 2005) 78, 686-693

E N D
Articles Acute serious and fatal reactions to contrast media: our current understanding • S K Morcos, FRCS, FRCR • British Journal of Radiology (2005) 78, 686-693 Adverse Reactions to Intravenous Iodinated Contrast Media: An Update • Saravanan Namasivayam MD, DNB, DHA, Mannudeep K. Kalra MD, DNB, William E. Torres MD and William C. Small MD, PhD • Current Problems in Diagnostic Radiology Volume 35, Issue 4 , July-August 2006, Pages 164-169
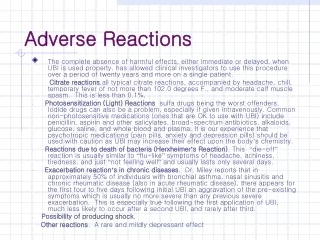
Introduction • unpredictable and not dose related • CM particles absorbed into the circulation • all the features of anaphylaxis • but IgE negative in most cases • developed within 5–30 min after exposure to CM • may present as generalized skin reactions, airway obstruction, angioedema or cardiovascular collapse • intermediate risk for anaphylaxis with CM
Prevalence of life threatening and fatal reactions to contrast media • severe and very severe reactions (IV push of CM) 0.22% and 0.04% after high-osmolar contrast media (HOCM) 0.04% and 0.004% after low-osmolar contrast media (LOCM) However no difference in fatal reactions (1:170 000) • UK & USA(FDA) (per million examinations) high with low osmolar CM 194 vs 44 for all reactions 37 vs 11 for severe reactions 3.9 vs 2.1 for fatal reactions. • high osmolar agents V.S.ioxaglate (a low osmolar ionic dimer) total reactions 194 vs 143 severe reactions 37 vs 34 fatal reactions 3.9 vs 6.4 • low osmolar non ionic CM is the best, besides no definite reduction in fatal reactions,
Risk factors • 1. A history of previous severe adverse reaction to a contrast agent 6 (both ionic and non-ionic CM) • 2. Asthma6~10 • 3. A strong history of allergic reactions to different substances (hay fever….) • 4. Treated with ß-adrenergic blockers and interleukin-2 (IL-2) acute adverse reactions to CM. (including the ophthalmic preparations) • 5. Iodinated CM 3 • 6. Female<-> the fatality rate :men with old age?! • 7. Race • 8. Malignant tumours an increase in histamine release • Pre-testing with an intravenous injection of a small amount of CM is not useful • High awareness !!
Table 1. European Society of Urogenital Radiology (ESUR) guidelines on prevention of generalized contrast medium reactions in adults
Pathophysiology of life threatening/fatal reactions to contrast media • adverse reactions to drugs type B reactions, not dose dependent and unpredictable • Aronson and Ferner: a new classification (DoTS) based on dose relatedness (Do), timing (T) and patient susceptibility (S) • drug (pharmacology and the dose dependence of its effects) • the properties of the reaction (time course of its appearance and its severity) • properties of the individual (the genetic, pathological and other biological differences that confer susceptibility) • Do-hyper susceptibility; T – first dose; S – not understood.
Pathophysiology • Type 1 hypersensitivity reaction (anaphylaxis) --- lack of consistency in demonstrating antibodies to CM • Within minutes • Chemotactic, vasoactive and spasmogenic compounds. leukotrienes, prostaglandins, enzymes • basophils and mast cells degranulation Histamine primary mediator ; intense immediate manifestations. (be reproduced by histamine infusion) vasodilatation, increasing vascular permeability edema contraction of smooth muscle cells bronchospasm ; increasing mucus secretion of airways recruit WBC additional waves of cytokines • direct effect of CM particles on these cells • non ionic monomers low levels of histamine release • Hyperosmolarity yes • Increasing the size and complexity of the molecule enhance the release of histamine
Pathophysiology--2 • Activation of factor XII (Hageman factor)kinin system production of bradykinin induce vasodilatation, bronchospasm and increase vascular permeability. • Bradykinin arachidonic acid cyclooxygenase and lipooxygenase pathways synthesis of PGs & LTs • Patients who are asthmatic or allergic increased concentration of factor XII products • CM DOESN’T act as haptens (non-reactive chemically) • p-I concept drugs may directly activate T cells via receptors that can interact with the drug. unlikely T cell VS. acute life threatening CM not clear • IgE antibodies? • Complement system (C3a, C4a and C5a) ? no significant difference
Diagnosis of serious or fatal reaction to contrast media • Histamine --- basophils and mast cells, tryptase---mast cells • Tryptase : 1–2 h after the reaction (not greater than 6 h) • Only very high concentrations of serum tryptase should be regarded specific • Histamine: 10 min to 1 h after the reaction • Methylhistamine, the main metabolite of histamine measured in urine • Specific IgE antibodies reliable drug RAST tests are not widely available • Positive intradermal tests some severe reaction to CM • it is advisable to measure serum tryptase routinely in severe or fatal patients (AMI or severe vasovagal attack may develop during examinations) • Post-mortem findings --- High level of seum tryptase, macroscopic findings including pulmonary oedema, signs of asthma (mucous plugging and/or hyperinflated lungs), petechial haemorrhages and pharyngeal/laryngeal oedema
Prevention of acute reactions to contrast media • Explained to the patient & the resuscitation team • Non-iodinated CM: 1. carbon dioxide (CO2) --- nausea, abdominal and leg pain may be observed with its administration 2. gadolinium based CM--- intravascular, no above 0.3 mmol kg–1 body weight induce nephrotoxicity (not sure) • Non-ionic contrast media (sure) • The prophylactic use of corticosteroids --- mechanism unclear • Antihistamines (H1 and H2) and ephedrine --- (not sure) • Corticosteroids complex with the cytoplasmic receptormigrate into the cell nucleus activate DNA dependent RNA synthesis accelerated formation of specific enzymes inhibitors take time 1. significant elevation in functional C1-esterase inhibitorlevels, 12 h after ; inhibits the activated form of factor XII 2. Decreased arachidonic acid from cell membranes production of PGs <s (not sure)
Prevention of acute reactions to contrast media-2 • fatality may still occur in patients who received pre-medication and low osmolar CM • Prompt recognition and treatment of adverse side effects to CM invaluable • never be left alone for at least 20 min after CM injection • the venous access • Emergency administration of contrast media in high-risk patients 1. pre-treatment with hydrocortisone, 200 mg intravenously, immediately, and every 4 h until the procedure is completed 2. diphenhydramine, 50 mg intravenously before the procedure 3. low osmolar non-ionic CM
Treatment of acute severe reactions to contrast media • Important first-line management 1. Adequate airway, oxygen supplementation, (adrenaline use) 2. IV physiological fluids, measuring BP &HR (most effective treatment for hypotension) 3. Adrenaline effective drug increases BP, reverses peripheral vasodilatation, decreases angioedema and urticaria, reverses bronchoconstriction, and produces positive inotropic and chronotropic cardiac effects (avoided in the pregnant patient) Only one concentration (1:1000) IM of 0.5 ml of 1:1000 adrenaline preparation IV IS NOT GOOD requires careful ECG monitoring (arrhythmia) • Antihistamine H1 receptor blockers reduce symptoms from skin reactions slow onset of action, and they cannot block “ ALREADY” events • H2-antagonists not essential • IV injection of high-dose corticosteroids an immediate stabilizing effect on the cell membrane second-line treatment. reducing delayed recurrent symptoms • Inhaled ß-2-adrenergic agonists (albuterol, metaproterenol and terbutaline) bronchodilating • Atropine blocks vagal stimulation of the cardiac conduction system. Large doses of aptropine (0.6–1.0 mg) are indicated
Table 2. First-line emergency drugs and instruments that should be in the room where contrast medium is injected
Table 3. Simple guidelines for first-line treatment of acute severe reactions to contrast media