Download
1 / 36
380 likes | 667 Vues
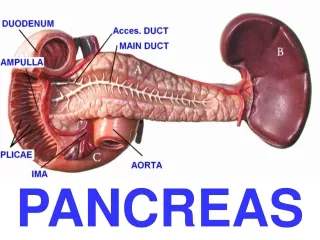
HISTOPATHOLOGY OF PANCREAS TRANSPLANTATION. Cinthia B. Drachenberg, M.D. University of Maryland School of Medicine. PANCREAS TRANSPLANTATION. 19,000, October 2002 (IPTR). PANCREAS TRANSPLANTATION. PANCREAS TRANSPLANTATION. Graft survival rates continue to improve

E N D
HISTOPATHOLOGY OF PANCREAS TRANSPLANTATION Cinthia B. Drachenberg, M.D. University of Maryland School of Medicine
PANCREAS TRANSPLANTATION • 19,000, October 2002 (IPTR)
PANCREAS TRANSPLANTATION
PANCREAS TRANSPLANTATION • Graft survival rates continue to improve • Simultaneous pancreas-kidney 85% • Pancreas after kidney 77% • Pancreas transplant alone 73% • Patient survival at one year >94%
HISTOPATHOLOGY OF PANCREAS TRANSPLANTATION • 12 years since the first percutaneous biopsies were performed (Allen et al. Transplantation 1991;51: 1213). • 1000 pancreas transplant bx at the Univ. of Maryland since 1992
Experimental models of acute pancreas allograft rejection • SEPTAL INFLAMMATION • VENOUS ENDOTHELIITIS AND INFLAMMATION OF DUCTS • ACINAR INFLAMMATION • INFLAMMATION OF ARTERIAL BRANCHES Allen et al: Am J Pathol 1991,138:303 Schulak et al: Surgery 1995,98:330. Steineger et al: Am J Pathol 1986,124:253. Carpenter et al: Transplantation 1989,48:764.
GRADING ACUTE REJECTION 0 No inflammation I Minimal septal inflammation II Venous endotheliitis III Acinar inflammation IV Arterial endotheliitis/ transmural arteritis V Parenchymal necrosis (Drachenberg et al.: Transplantation 1997;63:1579-86)
PANCREAS TRANSPLANT NEEDLE BIOPSY • Minimum tissue amount adequate for diagnosis in a needle biopsy: • Two lobules with associated septal tissue (arteries,veins, ducts). • H&E stained sections x3 • Masson’s trichrome stain • Unstained slides
Comparison between the first 100 and the last 100 biopsies First 100Last 100 Ac Rej Grade 0 15 29 Ac Rej Grade I 9 8 Ac Rej Grade II 12 8 Ac Rej Grade III 44 28 Ac Rej Grade IV 7 3 Ac Rej Grade V 5 0 Total Acute Rej 68% 39%
March 2002 April 2002 May 2002
PANCREAS TRANSPLANTS: GRADING OF CHRONIC REJECTION/GRAFT SCLEROSIS • Chronic rejection Grade 0 • Normal septa
PANCREAS TRANSPLANTS: GRADING OF CHRONIC REJECTION/GRAFT SCLEROSIS • Chronic rejection Grade I • Fibrosis in <30% of core • Center of the lobules intact
PANCREAS TRANSPLANTS: GRADING OF CHRONIC REJECTION/GRAFT SCLEROSIS • Chronic rejection Grade II • Fibrosis in 30-60% of core • Center of the lobules shows fibrosis
PANCREAS TRANSPLANTS: GRADING OF CHRONIC REJECTION/GRAFT SCLEROSIS • Chronic rejection Grade III • Extensive fibrosis in >60% of core • Minimal residual parenchyma
GRADO DE RECHAZO CRONICO EN RELACION AL TIEMPO DESDE EL TRANSPLANTE Y EN RELACION AL TIEMPO RESIDUAL DE FUNCION PANCREATICA
Comparison between the first 100 and the last 100 biopsies First 100Last 100 Ch Rej Grade I 3 14 Ch Rej Grade II 1 5 Ch Rej Grade III 0 4 Total Chronic Rej 4% 23%
HISTOPATHOLOGY OF PANCREAS TRANSPLANTATION • In comparison to other solid organ transplants, less is known. This pathology field continues to evolve together with the clinical and surgical advances in pancreas transplantation. • Has been a very important tool for the improvement of patient and graft outcomes, particularly in solitary pancreas transplantation.