NCI NCCCP Pilot Launch
NCI NCCCP Pilot Launch. Catholic Health Initiatives June 25-26, 2007 Presenters Debbi Honey, RN, MHA CHI Vice President Clinical Operations CHI liaison and contact for NCCCP Pilot Mark Krasna, M.D. Medical Director, St. Joseph Cancer Institute, Towson, MD

NCI NCCCP Pilot Launch
E N D
Presentation Transcript
NCI NCCCP Pilot Launch Catholic Health Initiatives June 25-26, 2007 Presenters Debbi Honey, RN, MHA CHI Vice President Clinical Operations CHI liaison and contact for NCCCP Pilot Mark Krasna, M.D. Medical Director, St. Joseph Cancer Institute, Towson, MD Principal Investigator, Catholic Health Initiatives NCCCP sites
Catholic Health Initiatives • Nation’s second largest Catholic healthcare system - not for profit • Facilities • 72 hospitals • 43 long-term, assisted-living and residential care facilities • 5 community-based health ministries • 19 States • Approximately 500,000 acute care admissions annually • Approximately 66,000 full and part-time employees • $8.8 billion in assets • $7.1billion in NPSR • 11% or $797 million as quantifiable community benefit (as percent of total revenues) Quantifiable community benefit (provided to the poor and broader community) as a percentage of total revenues: 11% or $797 million
Basis for Participation – Quality of Care • The broad geographic, size and service level diversity demands discipline and rigor to support quality care • Goal for all patients in a CHI facility to receive comparable high levels of quality care in services provided • System commitment to continual improvement in quality and patient safety • STEEEP • Central standardized information repository • Coordinated standard competency process • Active intra-facility collaboration increasing with oncology most active and engaged
Basis for Participation – Strategic Alignment • Mission and Vision • Creating Healthier communities • Commitment to serve disparate and underserved persons and populations • Supports strategic direction of organization • Focus on key service lines • Alignment and partnership with community providers • Enhancing and continually improving services available to patients in our communities
Basis for Participation – Strategic Alignment • Growth Strategy • Local– MBO oncology service line growth and development • National – Advancement of clinical services through an integrated approach across CHI • Innovation • Creating a culture that fosters innovation • Promoting transfer of new ideas and proven practices • Focused clinical service-line innovations: oncology, cardiology, ortho/neuro
Basis for Participation – Strategic Alignment • Research and Development • CHI Board initial commitment of $25M to new R&D function • Focus on creative approaches to transforming healthcare delivery • National partnerships and linkages will be key component • Integrated approach to clinical research activities across CHI
Basis for Participation – Distinctive Disparities • St. Joseph Medical Center, Towson, M People Served - 1.8 million • 35% are African American • Over 26.2% are older adults considered • Highest incidence of thoracic malignancies • Penrose-St. Francis Health Services, Colorado Springs, CO People Served – 564,776 • Medically Underserved designation in primary market area • Health professional shortage designation in primary care for low income populations. • Nebraska Hospitals – Good Samaritan Hospital, Kearney; St. Elizabeth Regional Medical Center, Lincoln; St. Francis Medical Center, Grand Island People Served – Collectively 920,000 • Large rural geographic areas with limited access due to distance and economic and personal issues. • Limited number of available trials makes Nebraska a prime target for an increase in both trial numbers and participant levels.
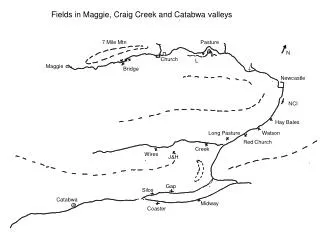
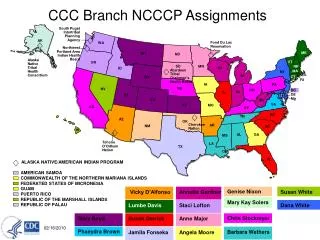
Basis for Participation – CHI MBO Complement to NCI Cancer Centers CHI Acute MBO Cancer Programs (40) Source: www3.cancer.gov/cancercenters/descriptionmap.html; modified on 4/09/06
Basis for Participation – System Advantages • Rural and Urban hospitals • National resources • Financial support • Clinical Expertise • Infrastructure for clinical and knowledge transfer • Infrastructure for standardized information in place to support outcome measurement • Leadership support, engagement and excitement at all levels of the organization • System-wide approach to service line strategies – example CHON
Challenges Collaboration Physician referrals Building confidence at “community” level Changing established referral patterns Disparate population participation Awareness Access Unanticipated resource needs Infrastructure Equipment Human Resources Opportunities Access to leading edge care for cancer patients Expansion of outreach opportunities Sharing of resources and scarce expertise Positively supports one of the system’s identified strategic service lines Local Considerations
“Extra Local” Considerations • Clinical Expertise – Sharing and Supporting • Specialty providers • Clinical and technical providers • Genetic counselors • Coordination with local agencies • Garnering collaboration between hospitals for service designation • Encourage and enhance ability to near “real-time” share lessons learned and best practices • Reputation for multidisciplinary care • Focus on innovation
Community Experience • Enjoy excellent reputation with consumers • Patients voice the desire to receive care at or near home when possible • High level patient satisfaction in facilities • State-of-the-art cancer facilities in several markets; commitment to enhance markets in development
Physician Experience • Medical staff actively involved • Believe hospitals/CHI are committed to quality and the community and actively partner with the facilities • Asked and participate in strategic planning activities • Actively participate in cancer committees at local level and participate in intra-facility • Complements existing private practice in local markets • Physician alignment – Strategies for recruiting and working with partner providers
NCCCP PILOT: NCI and CHI Synergy • Microcosm of U.S. Healthcare System • Geographic Diversity and Scope • Leadership Commitment • Commitment to Local Communities • National Infrastructure and Resources • National Information Strategy
System Dissemination and Integration • CHON • Development of a network for all CHI facilities with cancer programs to work together • Teleconferencing • Enhance ability to actively participate in clinical research and trials • Infrastructure enhancements
Catholic Health Oncology Network - CHON Research Multi-d Care • Become a highly sought after partner in the clinical development of new therapeutic approaches for cancer treatment • Establish multi-disciplinary care as the standard for treating oncology patients across CHI Goals:
CHON: Strategic Rationale Clinical Research Multi-disciplinary Care • Access to all therapeutic options; fully involving all team members improves quality of care • Cancer is by nature multidisciplinary, requiring services from several specialists • Multi-d teams allow the cancer program to address the continuum of patient care • Multiple benefits to building multidisciplinary oncology programs in a community setting: • For patients: make more informed decisions and receive better care (access, wait times) • For providers: provide better care, communication and work environment • For programs: build unique capabilities and market share • Providers that support clinical trials are viewed as being on the leading edge • Clinical research provides best cancer care • Clinical research across CHI is not organized, managed or marketed in a unified program • CHI is not benefiting from the advantages associated with being a leading research-focused system • CHI can address the many needs of research sponsors: • access to large, diverse pools of patients in a variety of disease areas • Participation by highly qualified, proven clinical investigators • Systems to acquire and deliver quality clinicaldatain a timely manner
Catholic Health Oncology Network - CHON • Business and Research Alignment: • The benefits to be gained from a CHON will be best realized by implementing systems and processes which: • Align CHI’s strategic, business and clinical objectives • Integrate and coordinate resources and activities to create efficiencies • Ensure properly shared infrastructures and uniform approaches to key activities • Foster timely and efficient communication and learning throughout the network • Enhance existing programs by complementing/partnering with other CHI sites/central office
The Cancer Institute at SJMC: The Mission • Create a coordinated team of dedicated specialists who willprovide the highest quality, compassionate care to patientswith malignancies, in an efficientand patient-friendly manner • Reinforce the positive clinical benefit of multidisciplinary care to patients, nurses and physicians
CHON: A Vision for the Future • Goals • Multidisciplinary care as the paradigm throughout CHI facilities • Provide access to multidisciplinary conferences • Facilitate live video/consultation or referral within the network to all specialties • Provide access to “state of the art care” at all rural CHI sites • Collaborate on new research initiatives • Offer state of the art access to clinical research trials • Collaborate with industry partners • Increase oncology market share
Questions ???