Download
1 / 43
430 likes | 433 Vues
Explore the rationale for investigating targeted therapeutic approaches and the latest clinical trial information in the management of IPF. Review current treatment options, their limitations, and future prospects.

E N D
IPF Disease Management Strategies With an Update on Clinical Trials and Ongoing Research
Objectives • Explain the rationale for investigating targeted therapeutic approaches to the management of IPF • Discuss the latest clinical trial information and research in the area of IPF • Review future treatment options for IPF
Current Therapies for IPF • Treatment remains controversial • Little good-quality evidence to support safety and efficacy of traditional agents (eg, immunosuppressive/ cytotoxic agents, corticosteroids) • Limited efficacy • Significant side effects • Limitations of older studies (eg, small sample size, variable study design, inconsistent diagnostic criteria) Collard HR, et al. Chest. 2004;125:2169-2174. ATS/ERS Consensus Statement. Am J Respir Crit Care Med. 2000;161:646-664. Richeldi L, et al. CochraneDatabase Syst Rev. 2003(3):CD002880; Davies HR, et al. Cochrane Database Syst Rev. 2003;(3):CD003134.
Effects of Conventional Treatment on Survival in IPF Patients 1.00 0.75 0.50 Probability of Survival Untreated (n = 82) Median survival = 1431 days 0.25 Treated (n = 82) Median survival = 1665 days 0.00 3500 3000 2500 500 2000 0 1500 1000 4000 Days of Follow-up Collard HR, et al. Chest. 2004;125:2169-2174.
Rationale for New Therapeutic Approaches to IPF Increased understanding of disease pathogenesis points to targeted therapies Limitations of older studies highlight need for prospective, randomized, controlled studies Rationale for New Therapeutic Approaches Evidence for survival benefit of IFN-g suggests new targets Shift in focus from inflammation to epithelial cells and myofibroblasts Brown KK, Raghu G. Clin Chest Med. 2004;25:759-772.
IPF Clinical Research Network: NHLBI Commitment Objective: • Establish a clinical research network of 6–7 clinical centers to design and conduct multiple therapeutic trials in newly diagnosed IPF patients • Evaluate potential therapeutic interventions • Establish a data coordinating center for the network http://grants.nih.gov/grants/guide. Accessed December 2004.
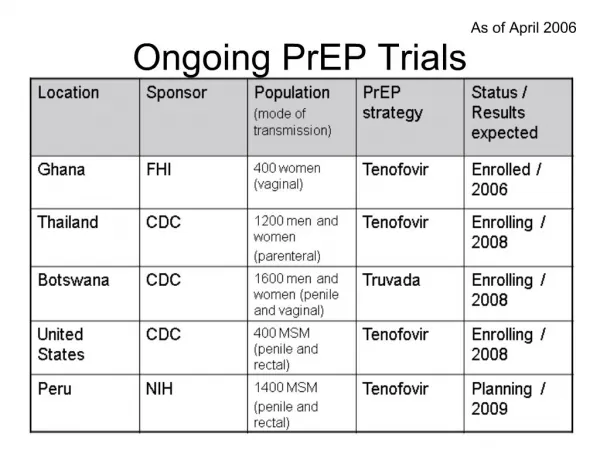
Recent and Ongoing Clinical Trials for IPF http://www.clinicaltrials.gov. Accessed December 2004. http:// www.coalitionforpf.org. Accessed December 2004. National Heart, Lung, and Blood Institute Strategic Plan. FY 2005-2009.
Biological Effects of Interferon Gamma • Interferon gamma (IFN-g) has pleiotropic effects: –Activates cell-mediated immunity –Inhibits fibroblast proliferation –Reduces collagen synthesis –Attenuates fibrosis in animal models –Reduces tissue myofibroblast numbers Raghu G, Chang J. Clin Chest Med. 2004;25:621-636. Selman M, et al. Drugs. 2004;64:405-430. Raghu G, et al. New Engl J Med. 2004;350:125-133.
Clinical Trials of Interferon Gamma-1b GIPF-001 Trial Raghu G, et al. N Engl J Med. 2004;350:125-133. http:// www.clinicaltrials.gov. Accessed December 2004.
Lung Function and Survival Outcomes in GIPF-001 Lung Function (FVC) Survival* Intention-to-treat (N = 330) 75 1.0 IFN -1b P = NS 70 P = 0.08 0.8 65 IFN -1b Probability of Survival Placebo Mean % Predicted FVC 60 0.6 Placebo IFN -1b IFN -1b 55 Placebo Placebo 50 0.4 0 100 200 300 400 500 600 0 12 24 36 48 60 72 Day Week Slide courtesy of Steven D. Nathan, MD. *Raghu G, et al. N Engl J Med. 2004;350:125-133.
GIPF-001 Study: Mortality 28 16 King TE Jr, et al. Chest. 2005;127:171-177.
Likelihood of MortalityMultivariate Analysis Baseline Risk Factors Lynch D, et al. Paper presented at: 2004 American Thoracic Society; 2004; Orlando, Florida. Abstract A706.
Mortality by Baseline FVC King TE, et al. Chest. 2005;127:171-177.
Predictors of Near-Term MortalityMultivariate Analysis Using Dynamic Variables Martinez FJ, et al. Ann Intern Med. In review.
Key Implications of GIPF-001 Trial • Potentially significant survival benefit in mild-to-moderate patients could not be ruled out • Preliminary evidence of improved survival in the absence of any effect on lung function • Survival as a key endpoint for future clinical trials • Risk of death is similar across various degrees of disease severity • Stability of lung function does not necessarily mean stability of disease Raghu G, et al. N Engl J Med. 2004;350:125-133. King TE, et al. Chest. 2005;127:171-177.
Clinical Trials of Interferon GIPF-002 (complete) Strieter RM, et al. Am J Respir Crit Care Med. 2004;170:133-140.
Key Implications of GIPF-002 Trial • IFN g-1b appears to favorably affect multiple biologic pathways in IPF patients, including: • Inhibition of fibrosis molecules, growth factors, inflammatory/ angiogenic ENA-78/CXCL5 • Enhanced expressionof immunomodulatory, antiangiogenic, and antimicrobial molecules ITAC/CXCL11 • These activities may translate into beneficial clinical effects on fibrosis and/or antimicrobial defense in IPF patients Strieter RM, et al. Am JRespir Crit Care Med. 2004;170:133-140.
Hellenic IPF Study: Interim Analysis of Survival 1.0 0.8 0.6 Survival Distribution P = 0.01 Log-rank test 0.4 IFN -1b (n = 27) 0.2 Colchicine (n = 15) 0 0120 240 360 480 600 720 840 960 Time (days) Slide courtesy of V. Polychronopoulos and D. Bouros on behalf of the Hellenic Interstitial Lung Disease Group; Antoniou KM, et al. Abstract presented at ATS International Conference May 2003, Seattle, WA.
Clinical Trials of Interferon The INSPIRE Trial (ongoing) http:// www.clinicaltrials.gov. Accessed December 2004.
The Role of N-acetylcysteine (NAC) in IPF • Increased levels of reactive oxygen species in IPF lung • NAC acts as anti-oxidant to scavenge hydrogen peroxide • NAC is a precursor to glutathione (an anti-oxidant), which is deficient in IPF • Preliminary evidence from a small (n = 18) proof-of-concept study suggests NAC in addition to immunosuppressive therapy increases levels of reduced glutathione and improves pulmonary function in IPF patients Behr J, et al. Am J Respir Crit Care Med. 1997;156:1897-1901. http://www.chestnet.org. Accessed November 2004. National Heart, Lung, and Blood Institute Strategic Plan. FY 2005-2009.
Phase 3 Clinical Trial of NAC for IPF The IFIGENIA Trial Behr J. Paper presented at: 2004 American Thoracic Society; 2004; Orlando, Florida. Abstract B73.
Preliminary Results of IFIGENIA Trial • Patient disposition: of 184 randomized, 57 (71%) NAC-treated patients, and 51 (68%) placebo-treated patients completed the trial • Preliminary results: • NAC-treated patients showed less decline in FVC and DLco than placebo-treated patients • Generally no effect on secondary efficacy endpoints Demedts M, et al. Poster presented at: 14th ERS Congress; 2004; Glasgow, Scotland. Poster 4077, Poster 4078. Behr J, et al. Poster presented at: 14th ERS Congress; 2004; Glasgow, Scotland. Poster 4079. National Heart, Lung, and Blood Institute Strategic Plan. FY 2005-2009.
IFIGENIA Study: Results • N = 184 pts enrolled from March 2000–June 2002 • N = 155 suitable for final analysis • Demographics • Age = 63 (mean age) • 47% surgical lung biopsy • 52% diagnosed within 6 months of enrollment • Male = 71% • FVC = 65% • TLC = 62% • DLCO = 44% • PaO2 maximal exercise = 53 mm Hg Behr J. Paper presented at: 2004 American Thoracic Society; 2004; Orlando, Florida. Abstract B73. Slide courtesy of Steven D. Nathan, MD
IFIGENIA Study: Results FVC DLCO 8% 24% Pred/Aza/NAC Pred/Aza P < 0.05 P < 0.005 0 12 0 6 6 12 Month Month Behr J. Paper presented at: 2004 American Thoracic Society; 2004; Orlando, Florida. Abstract B73. Slide courtesy of Steven D. Nathan, MD.
The Role of Endothelins in IPF http://www.actelion.com/uninet/www/www_main_p.nsf/Content/Tracleer+Healthcare+Professionals. Accessed January 2005. Selman M, et al. Drugs. 2004;64:405-430.
Phase 2/3 IPF Clinical Trials The BUILD Trial (completed) http:// www.clinicaltrials.gov. Accessed December 2004.
Pirfenidone in IPF • 5-methyl-1-phenyl-2-(1H)-pyridone • Has antifibrotic activity in vivo and in vitro • Inhibits TGF-β-induced collagen synthesis in IPF-derived lung fibroblasts • Inhibits mitogenic effects of profibrotic cytokines on lung fibroblasts CH3 N O http:// jcem.endojournals.org/cgi/content/full/83/1/219/F1. Accessed January 2005. Raghu G, et al. Am J Respir Crit Care Med. 1999;159:1061-1069.
Phase 2/3 Trials of Pirfenidone Raghu G, et al. Am J Respir Crit Care Med. 1999;159:1061-1069. Azuma A, et al. Am J Respir Crit Care Med. 2005;doi:10.1164.
Pirfenidone Phase 3 Trial Proposed Trial Design Data on file with InterMune.
The Role of Tumor Necrosis Factor-alpha in IPF • TNF-a: • Pleiotropic cytokine • May stimulate fibroblast proliferation and collagen gene expression through TGF-b and/or PDGF • Enhanced expression in patients with IPF • In an open-label, pilot study in 9 IPF patients, etanercept (TNF-a antagonist) appeared to be well tolerated • Suggestion of improvement in FVC, DLCO, P(A-a)O2 in some patients ATS Abstract 2001. Niden A. et al. ATS Abstract 2002. Niden A. et al Brown KK. Clin Chest Med. 2004;25:759-772
Phase 2/3 IPF Clinical Trials Etanercept http:// www.clinicaltrials.gov. Accessed December 2004. http:// www.coalitionforpf.org. Accessed December 2004.
Role of Imatinib Mesylate in IPF • Antineoplastic agent • Targets the c-Abl gene, which initiates the destructive, abnormal growth of lung tissue • Inhibits profibrotic growth factors TGF-b and PDGF • Significantly inhibits lung fibrosis in bleomycin-induced pulmonary fibrosis in mice Daniels CE, et al. J Clin Invest. 2004;114:1308-1316.
Phase 2 IPF Clinical Trials Imatinib Mesylate Trial (ongoing) http://www.coalitionforipf.org/IPFResearch. Accessed December 2004.
FG-3019: Phase 1 Trial for IPF • Human monoclonal antibody against connective tissue growth factor (CTGF), a growth factor that plays a key role in fibrosis • Reduces scarring and excess deposition of ECM in preclinical models • Phase 1 trial of FG-3019 • Evaluated safety, pharmacokinetics, immunogenicity in patients with IPF • Patients treated with FG-3019 at 1, 3, or 10 mg/kg by IV infusion for 2 hours • FG-3019 was safe and well tolerated • Phase 2 trial planned for 2005 Coalition for Pulmonary Fibrosis. ACT. October-December 2004. Mageto Y, et al. CHEST. October 26, 2004; Seattle, WA.
Therapeutic Approaches to IPF: Where We’ve Been, Where We’re Going… Immunomodulation Anti-inflammatory Anti-fibrotic Future Antiproliferative Immunosuppression Anti-oxidant IFN-g 1b Etanercept Pirfenidone FG-3109? Statins? LO Inhibitors? Combo Tx? Colchicine D-penicillamine Imatinib Bosentan Corticosteroids azathioprine cyclophosphamide NAC glutathione 1950s 1990s 2005
Guidelines for Transplant Referral for IPF • Symptomatic, progressive disease persists despite steroids or other immunosuppressive drug therapy • Withdraw steroids or other cytotoxic agents if no meaningful benefit has been achieved • Vital capacity < 60%–70% predicted and/or the diffusing capacity (corrected for alveolar volume) < 50%–60% predicted • Consider referral to transplant center, although patient may be minimally symptomatic • New guidelines pending publication Maurer JR. Am J Respir Crit Care Med. 1998;158:335-339.
International Society for Heart and Lung Transplantation Trulock EP, et al. J Heart Lung Transplant.2004;23:804-815. Adapted from website: www.ishlt.org. Accessed January 2005. Adult Lung TransplantationKaplan-Meier Survival by Diagnosis(Transplants: January 1990 – June 2002) 100 COPD (N= 4,955) IPF (N= 2,119) PPH (N= 737) Sarcoidosis (N = 317) 75 Survival (%) 50 25 HALF-LIFE COPD: 4.6 Years; IPF: 3.4 Years; PPH: 4.0 Years; Sarcoidosis: 3.8 Years 0 0 1 2 3 4 5 6 7 8 9 10 Years
International Society for Heart and Lung Transplantation Trulock EP, et al. J Heart Lung Transplant.2004;23:804-815. Adapted from website: www.ishlt.org. Accessed January 2005. Adult Lung TransplantationKaplan-Meier Survival by Procedure Type (Transplants: January 1990 – June 2002) Diagnosis: IPF 100 75 Survival (%) 50 N = 18 N=18 25 Single Lung (N = 1,645) Double Lung (N = 474) N = 22 P = 0.5 0 0 1 2 3 4 5 6 7 8 9 10 Years
Lung Allocation System • Major changes planned for 2005 • Allocation will be based on scores for: • Estimated transplant benefit (survival after 1 year) • Estimated mortality (at 1 year) without transplant http://www.ishlt.org. Accessed December 2004. Thabut G, et al. J Thorac Cardiovasc Surg. 2003;126:469-475. http://www.unos.org/SharedContentDocuments/Lung_Patient.pdf. Accessed December 2004.
On the Waitlist FVC PA systolic O2 required at rest Age BMI IDDM NYHA class 6MWT distance Ventilator use Diagnosis After Lung Transplant FVC PCW pressure > 20 Ventilator use Age Creatinine NYHA class Diagnosis Factors Used to Predict Death
Survival Benefit of Lung Transplantation in IPF Patients • Most common indication for adult lung transplantation (17%) after COPD/emphysema (39%) • 50% survival at year 3 • 46 IPF patients accepted for lung transplantation during a 12 year period showed: • Survival of 79% at year 1, 63% at year 2 and 39% at year 5 • Mean waiting time for organ: 51 days • Risk of death reduced by 75% • (95% CI = 8%–86%; P = 0.03) http://www.ishlt.org. Accessed December 2004. Thabut G, et al. J Thorac Cardiovasc Surg. 2003;126:469-475.
Nonpharmacological and Additional Management Strategies of IPF • Supplemental oxygen • Pulmonary rehabilitation • Improvement in general and disease-specific health status • Increase exercise tolerance • End-of-life care and use of palliative care • Screen for pulmonary hypertension, obstructive sleep apnea, cough, gastroesophageal reflux disease, and coronary artery disease Adapted from http://www.lungusa.org. Accessed December 2004.
Take Home Messages • Little good-quality evidence supports the safety and efficacy of traditional therapies for IPF • Survival and 10% improvement in FVC may be key endpoints for future clinical trials • Evolving concepts regarding disease pathogenesis point to new therapeutic targets • Ongoing clinical trials may lead to therapies targeting multiple pathogenic mechanismsmany of these trials are still accepting new patients • Lung transplantation can significantly reduce the risk of death for IPF patients • Nonpharmacological treatments are important adjuncts to pharmacotherapy for IPF