ACC/AHA Guidelines STEMI
ACC/AHA Guidelines STEMI. DR RAJESH K F. Applying Classification of Recommendations and Level of Evidence. Applying Classification of Recommendations and Level of Evidence. Evolution of Guidelines for STEMI. 1990 ACC/AHA MI R Gunnar

ACC/AHA Guidelines STEMI
E N D
Presentation Transcript
ACC/AHA Guidelines STEMI DR RAJESH K F
Applying Classification of Recommendations and Level of Evidence
Applying Classification of Recommendations and Level of Evidence
Evolution of Guidelines for STEMI • 1990 ACC/AHA MI R Gunnar • 1996 ACC/AHA review MI T Ryan • 1999 ACC/AHA update MI T Ryan • 2004 ACC/AHA review STEMI E Antman • 2007 ACC/AHA update STEMI E Antman • 2009 ACC/AHA update STEMI & PCI F Kushner
Prehospital issues • Management in ED • Management in hospital • Long term management
Prehospital Chest pain Evaluation and Treatment • Prehospital EMS providers should administer 162-325 mg of non enteric coated aspirin (chewed) to suspected STEMI patients • All ACLS providers perform and evaluate ECGs of suspected STEMI patients
Prehospital Fibrinolysis • Establishment of prehospital fibrinolysis protocol is reasonable in 1) when physicians are present in ambulance or 2)well organized EMS systems(if transport time more than 60 min)
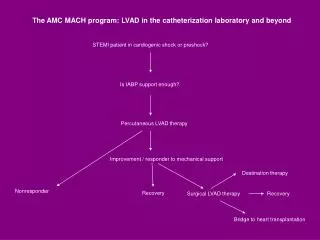
Prehospital Destination Protocols • Patients with STEMI who have cardiogenic shock and are <75yrs should be brought immediately or secondarily transferred to facilities capable of PCI and CABG if it can be performed within 18 hrs of shock (SHOCK TRIAL) • >75yrs and high risk of dying
Patients with STEMI who have contraindications to fibrinolysis should be brought immediately or secondarily transferred to facilities capable of PCI and CABG • (Door to departure time <30min)
It is reasonable to transfer high risk patients who receive fibrinolytic therapy at non-PCI capable facility to a PCI-capable facility as soon as possible where either PCI can be performed when needed or as a pharmacoinvasive strategy. • Consideration should be given to initiating a preparatory antithrombotic (anticoagulant plus antiplatelet) regimen prior to and during patient transfer (CARESS-IN-AMI,TRANSFER-AMI)
Pathway: Triage and Transfer for PCI (in STEMI) STEMI patient who is a candidate for reperfusion Initially seen at a non-PCI capable facility Initially seen at a PCI capable facility Initial Treatment with fibrinolytic therapy (Class 1, LOE:A) Send to Cath Lab for primary PCI (Class I, LOE:A) Transfer for primary PCI (Class I, LOE:A) HIGH RISK Transfer to a PCI facility is reasonable for early diagnostic angio & possible PCI or CABG (Class IIa, LOE:B), High-risk patients as defined by 2007 STEMI Focused Update should undergo cath (Class 1: LOE B) NOT HIGH RISK Transfer to a PCI facility may be considered (Class IIb, LOE:C especially if ischemic symptoms persist and failure to reperfuse is suspected), At PCI facility, evaluate for timing of diagnostic angio Prep antithrombotic (anticoagulant plus antiplatelet) regimen Diagnostic angio Medical therapy only PCI CABG
Options for Transport of Patients With STEMI and Initial Reperfusion Treatment Hospital fibrinolysis: Door-to-Needle within 30 min. Not PCI capable Call 9-1-1 Call fast • EMS on-scene • Encourage 12-lead ECGs. • Consider prehospital fibrinolytic if capable and EMS-to-needle within 30 min. Inter-Hospital Transfer Onset of symptoms of STEMI 9-1-1 EMS Dispatch EMS Triage Plan PCI capable GOALS 5 min. 8 min. EMS Transport Patient EMS Prehospital fibrinolysis EMS-to-needle within 30 min. EMS transport EMS-to-balloon within 90 min. Patient self-transport Hospital door-to-balloon within 90 min. Dispatch 1 min. Golden Hour = first 60 min. Total ischemic time: within 120 min.
Initial patient evaluvation • Targeted history • Physical examination including focused and limited neurological examination to look for prior stroke or cognitive defects prior to thrombolysis
ECG • A 12 lead ECG should be performed within 10 min • If not diagnostic and patient is symptomatic, serial ECGs at 5to10min or continuous ST segment monitoring • In patients with IWMI, Rt sided ECG leads should be obtained
Laboratory examinations • Should be performed but should not delay implementation of reperfusion therapy • Serial biomarker measurements useful to provide supportive noninvasive evidence of reperfusion • Serial biomarker measurements should not be relied on to diagnose reinfarction in 18 hrs after onset of STEMI
Cardiac Biomarkers in STEMI 100 50 Cardiac troponin-no reperfusion 20 Cardiac troponin-reperfusion CKMB-no reperfusion Multiples of the URL 10 CKMB-reperfusion 5 2 Upper reference limit 1 0 1 2 3 4 5 6 7 8 URL = 99th %tile of Reference Control Group Days After Onset of STEMI Alpert et al. J Am Coll Cardiol 2000;36:959. Wu et al. Clin Chem 1999;45:1104.
Imaging • Should have a portable CXR but should not delay reperfusion unless AD is suspected • Portable CXR,TTE or TEE ,contrast CT or MRI should be used to differentiate STEMI from AD if not clear initially
Portable echo in ED is reasonable to • Clarify diagnosis of STEMI • Risk stratification • Diagnosis confounded by LBBB or pacing • Suspicion of PWMI with anterior ST depression • Mechanical causes of failure or shock
Routine measures Oxygen • Supplemental oxygen should be administered to patients with SaO2<90% • It reasonable in all patients in first 6hrs
Nitroglycerin • Patients with ongoing pain should receive s/l NTG (.4mg) for a total 3 doses • IV NTG indicated for ongoing pain control of hypertension pulmonary congestion
Nitrates should not be administered when SBP<90mmhg SBP<30mmhg below baseline Severe bradycardia (<50) Tachycardia(>100) Suspected RV infarction Those received PDE inhibitor in 24 hrs (48hrs for tadalafil)
Analgesia • Morphine sulfate(2-4mg IV with increments 2-8mg IV 5 to 15 min intervals) is the choice • Patients taking NSAIDS should be discontinued due to increased risk of mortality ,reinfarction , HTN,HF and myocardial rupture • (ExTRACT TIMI25)
Aspirin • Aspirin should be chewed by patients who have not taken ,initial dose • 162 • 325 • maintenance dose of 75 to 162 mg should be given indefinitely after STEMI to all patients without a true aspirin allergy
For all post PCI STEMI patients stented without aspirin resistance ,allergy or increased risk of bleeding • 162.5 to 325 mg od for 1month after BMS • 3months after SES • 6months after PES • After which 75 to 162 mg/d and continue indefinitely. • if concerned about risk of bleeding 75 to 162 mg is reasonable in initial period
Beta blocker • Oral beta blocker therapy should be initiated in 24hrs to those who not have Signs of HF E/O low out put state Increased risk for cardiogenic shock >70yrs,SBP< 120,HR>110 or< 60 or Increased time since onset of symptoms • Other relative CI PR>.24sec 2nd or 3rd degree HB Active asthma Reactive airway diseases
It is reasonable to administer IV BB at the time of presentation to patients who are hypertensive without any above contraindications • Continue indefinitely • (COMMIT/CCS 2)
Reperfusion • STEMI patients presenting to a facility without PCI or capability to transfer for PCI in 90 min should undergo fibrinolysis in 30 min • ( compared with fibrin specific agent PCI may not reduce mortality if delay>60min)
Pharmacological reperfusion • In the absence of contraindications fibrinolytic therapy should be administered if symptom onset within prior 12hrs and ST elevation >1mm in 2adjuscent limb leads or 2 contiguous chest leads • New or presumably new LBBB
It is reasonable if STEMI beginning within prior 12 to 24 hrs who have continuing chest discomfort and ST elevation • It is reasonable if findings consistent with true PWMI
The occurrence of a change in neurological status during or after reperfusion therapy particularly within 24hrs is considered to be ICH unless proved otherwise . Fibrinolytic, antiplatelet and anticoagulants should be discontinued until brain imaging disproves ICH
Primary PCI • Patients with STEMI or MI with new or presumably new LBBB • PCI of infarct related artery within 12hr of symptom onset • Door to balloon time <90min • Person skilled in procedure(>75PCI/yr) • Supporting lab (>200PCI/yr of which 36 primary) • Cardiac surgical backup available
STEMI patients presenting to hospital with PCI capability should be treated with primary PCI in 90 min • If symptom duration is within 3hrs and expected DB-DN is <1hr primary PCI >1hr fibrinolysis • >3hrs-primary PCI is generally preferred with a goal of DB time <90 min
<75yrs who develop shock within 36hrs of MI and suitable for revascularization that can be performed within 18hrs of shock • Severe CHF and/or pulmonary edema(killip3) and onset of symptoms within 12hrs (DB<90 min)
Primary PCI is reasonable for selected patients >75yrs who develop shock ….. • It is reasonable if onset of symptoms within prior 12 to 24hrs and severe CHF or hemodynamic or electrical instability or persistent ischemic symptoms
Should not be performed in non infarcted artery • Should not be performed in asymptomatic patients >12hr after onset if they are hemodynamically and electrically stable
In fibrinolytic ineligible patients • It should be performed who present in12hrs • It is reasonable who present in12 to 24hrs and one of the following severe CHF hemodynamic or electrical instability persistent ischemic symptoms
Facilitated PCI • Regimens other than full dose fibrinolytic therapy might be considered when all of the following are present high risk patient PCI not available in 90 min bleeding risk is low • Facilitated PCI with full dose fibrinolysis is harmful • (ASSENT-4PCI,FINESSE )
Rescue PCI • A strategy of CAG with intent to perform PCI (or emergency CABG) is recommended for patients after fibrinolysis, have any one of following <75yrs who develop cardiogenic shock within 36hrs of MI and suitable for revascularization severe CHF or and /pulmonary edema (killip3) hemodynamicallycompromising ventricular arrhythmia
Is reasonable for patients after fibrinolysis in patients >75yrs who develop cardiogenic shock and suitable for revascularization • It is reasonable for patients with one of the following hemodynamic or electrical instability or persistent ischemic symptoms
It is reasonable in failed fibrinolytic therapy(<50% ST resolution in lead with worst initial elevation) and moderate to large area of myocardium at risk (AWMI,IWMI +RVMI , precordial ST depression) • (REACT)
PCI after successful fibrinolysis or no reperfusion • PCI of totally occluded IRA >24hrs after STEMI not recommended in asymptomatic with SVD or DVD if hemodynamically and electrically stable and do not have E/O ischemia
Ancillary therapy • Patients undergoing reperfusion with fibrinolytics should receive anticoagulant therapy for minimum 48hrs • And preferably for duration of index hospitalization ,up to 8days (UFH is not recommended after 48hrs due to risk of HIT) • UFH should be given intravenously in (dose 60U/kg max 4000U bolus, 12U/kg/hr max 1000/hr)(APTT 1.5 to 2 x control)
Enoxaparin( SCr <2.5 in male and 2 in female) (ExTRACT TIMI 25) • <75yrs dose 30mg IV bolus ,1mg/kg scbd • >75 0.75mg/kg scbd • Cr cl<30 1mg/kg od Fondaparinux(SCr<3mg) 2.5mgIV then 2.5mg sc od (OASIS 6)
It is reasonable for patients do not undergo reperfusion therapy to be treated with anticoagulant therapy (non UFH regimen),dose time similar • (CREATE,OASIS-6)
IIa IIa IIa IIa IIb IIb IIb IIb III III III III I I I IIa IIa IIa IIa IIb IIb IIb IIb III III III III I I I IIa IIa IIa IIa IIb IIb IIb IIb III III III III I I I B For patients proceeding to primary PCI • For prior treatment with UFH, additional boluses should be administered as needed to maintain therapeutic APTT(200/250) taking into account whether GP IIb/IIIa receptor antagonists have been administered • Bivalirudin is useful as support for primary PCI with or without prior treatment with heparin. (HORIZONS-AMI)
Prior enoxaparin If last sc dose in 8hrs no additional dose If last sc dose in 8to 12hrs IV 0.3 mg/kg
Prior fondaparinux • additional IV anticoagulant possessing anti IIa activity taking into account, whether GPIIb/IIIa RA given • Because of the risk of catheter thrombosis fondaparinux should not be used as sole anticoagulant