Download
1 / 21
240 likes | 654 Vues
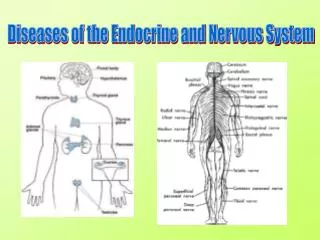
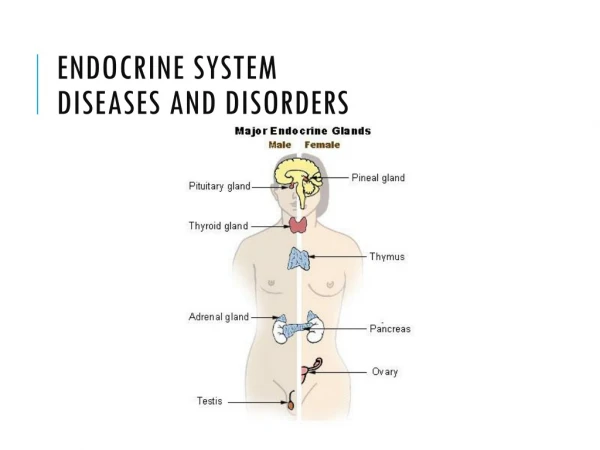
Diseases and Disorders of the Endocrine System. Abnormalities of Growth Hormone Secretion. Panhypopituitarism – refers to decrease secretion of all the anterior pituitary hormones Causes – congenital pituitary tumor (that destroys the pit)

E N D
Abnormalities of Growth Hormone Secretion • Panhypopituitarism – refers to decrease secretion of all the anterior pituitary hormones • Causes – congenital pituitary tumor (that destroys the pit) • Can occur slowly or suddenly @ anytime during life
Dwarfism • General deficiency of ant.pit. secretion during childhood • All body parts develop in proportion, but rate of development greatly decreased (10 yr. old w/body of 4-5yr. , 20 yr. old-body 7-10 yr. old) • Never goes thru puberty (doesn’t secrete enough gonadotropic hormones to dev adult sex functions) • 1/3 dwarfs only GH def. –do mature sexually and can reproduce. • Dwarfs w/pure GH def. can be cured with Human Growth hormone, if treated early in life.
Panhypopituitarism in adult • 1st occurs in adulthood • Causes: 1. tumerous conditions may compress pit. gland until ant.pit. cells are destroyed. • 2. thrombosis (clot)of pit. blood vessels (occasionly occurs in childbirth if mother develops circulatory shock. • General effects: 1.hypothyriodism 2. depressed production of glucocorticoids by adrenals 3. suppressed secretion of gonadotropichorm. So that sexual functions are lost. • Picture –lethargic person(lack TH) who is gaining wt. (b/c lack fat mobilization by GH, ACTH, ACH and TH) and has lost all sexual functions. • Treatment: adrenocortical and thyroid hormones
Gigantism • Growth hormone-producing cells of ant. Pit. Becomes excessively active and sometimes tumors occur in gland , resulting in lg. quantities of GH produced. • All body tissues grow rapidly, including bones • If occurs before adolescence (before epiphyses of long bones become fused w/shafts) ht. increases so that person becomes a giant (up to 8 ft. tall) • Usually caused by a pituitary tumor that grows until gland is destroyed (usually causes death in early adulthood) • Once gigantism is diagnosed further effects can be blocked by microsurgical removal of tumor or irradiation of pit. gland.
Acromegaly • Condition occurring from pituitary tumor after adolescence (after epiphyses of long bones have fused w/shafts) • Person cannot grow taller but bones become thicker and soft tissues continue to grow. • Marked enlargement of bones of hands and feet and in membranous bones (including: cranium, nose, bosses on forehead, supra-orbital ridges, lower jawbone and portions of the vertebrae) • Picture a person whose lower jaw protrudes forward, forehead slants forward, nose 2x nl., feet size 14 or larger, fingers extremely thickened, hands twice nl size and hunched back (kyphosis). Also, soft tissue organs such as tongue, liver and kidneys become greatly enlarged.
Diseases of thyroidHyperthydroidism • Graves disease-an autoimmune disorder in which antibodies attack the thyroid causing excessive hormone production (can secrete TH @ rates 5-15x nl) • Thyroid gland increases in size to 2-3x nl (goiter) + # of cells increases • One of most common hormonal disorders, especially in women age 20-50. ¾ of hyperthyroid cases are due to Graves’ disease. • Less common cause are nodules (sm. lumps) in the gland and thyroid adenomas (tumor which develops in the thyroid tissue) – secrete lg. quantities of TH.
Symptoms of hyperthyroidism: • 1. increased metabolic rate • 2. weight loss (mild to extreme) d/t increased energy usage • 3. rapid irregular heartbeat • 4. trembling (hand tremors) • 5. increased sweating • 6. anxiety and a high state of excitability • 7. intolerance to heat • 8. extreme fatigue with insomnia • 9. muscle weakness • 10. varying degrees of diarrhea • 11. exophthalmos (protrusion of eyeballs) (sometimes optic nerve is stretched causing visual damage, dry eyes and infections) • 12. goiter (enlarged thyroid causing swelling in the neck) • Treatment: surgical removal of thyroid gland. Also injection of radioactive iodine to destroy most of the secretory cells of thyroid gland.
Hypothyroidism • The thyroid hormones(tri-iodothyronine and thyroxine) are under-produced. Since they govern the speed of many metabolic processes, their lack lead to a slowing down of body functions. • Usual cause is Hashimoto’s thyroiditis –autoimmune condition in which antibodies develop which cause inflammation->progressive deterioration-> fibrosis of gland with resultant decrease or absent secretion of TH. • Endemic colliod goiter –goiter caused by iodine deficiency (50mg iodine required /yr. for formation adequate quantities TH). (Great Lakes reg., Swiss Alps and Andes + underdeveloped areas – insufficient iodine in soil to get this amt.) - iodized salt • Thyroid may increase 10-20x normal size
Symptoms of hypothyroidism • 1. fatigue and extreme somnolence (12-14 hrs./day) • 2. muscle sluggishness • 3. slowed heart rate • 4. weight gain • 5. constipation (slow bowel activity) • 6. mental sluggishness • 7. thickened skin • 8. thinned hair • 9. hoarse voice • 10. myxedema – in severe cases (edematous appearance t/o body)
Myxedema • Develops in patients with almost total lack of thyroid hormone function. • Characterized by: bagginess under eyes, swelling of face, non-pitting edema • Many hypothyroid pts., especially those with myxedema develop atherosclerosis which results in PVD, deafness and CAD and early death.(lack TH increases blood cholesterol d/t altered fat and cholesterol metabolism & decreased liver excretion ) • Treatment: daily ingestion of a tablet of thyroxine. (results in such complete normality – formerly myxedematous pts. have lived into their 90’s after more than 50 yrs of treatment)
Cretinism • Extreme hypothyroidism during fetal life, infancy or childhood. • Characterized by: failure of body growth and mental retardation • Causes: 1. congenital lack of thyroid gland (congenital cretinism) • 2.failure of thyroid gland to produce TH from genetic defect or iodine lack in diet (endemic cretinism) • Short, stocky appearance. Occasionally tongue so large it obstructs swallowing and breathing • Treatment: adequate iodine or thyroxine therapy causes normal return of physical growth, but unless treated within few weeks after birth, mental growth remains retarded.
Hypoadrenalism-Addison’s disease • Failure of the adrenal cortices to produce adrenocortical hormones • Cause: autoimmunity against the cortices which results in atrophy of the adrenal cortices. (80%) Also caused by invasion of adrenal cortices by cancer. • Disturbances: • 1. mineralcorticoid def.- lack of aldosteronedec. renal tubular Na+ reabsorption – allows Na+, Cl- and water to be lost in urine -> plasma vol. decrease and decreased C.O. -> pt. dies of shock.(4 days-2 wks. after cessation of mineralcorticoids). • 2. glucocorticoid def. – impossible to maintain nl blood glucose levels between meals (b/c can’t synthesize glucose by glucogenesis) muscle weakness (can’t get protein and fat from tissues) , and highly susceptible to deteriorating effects of stress (mild URI can cause death) • 3. melanin pigmentation – of mucus membranes and skin. (b/c cortisol secretion is depressed-> nl neg. feedback to hypothalamus and ant pit depressed -> allows increased rate ACTH and MSH secretion -> increased melanin • Without treatment, dies within days to weeks d/t circ. shock and weakness • Treatment: small quantities of mineralcorticoids and glucocorticoids daily. Need to increase gluco. (often 10x nl) to prevent Addisonian crisis(severe debility with critical need for gluco. In times of stress)
Hyperadrenalism-Cushing’s syndrome • Hypersecretion by adrenal cortex and characterized by high plasma levels of ACTH and cortisol • Causes: 1. adenoma of anterior pituitary • 2. abnl function of hypothalamus • 3. ectopic secretion of ACTH by tumor elsewhere in body • 4. adenoma of adrenal cortex • 5. when lg. ants of glucocorticoids are administered over prolonged periods for therapeutic purposes (ie. Chronic inflammation such as RA)
Characteristics of Cushing’s • Buffalo torso (mobilization fat from lower part of body to thoracic and upper a abdomen) • Moon face (facial edema – steroids) • Hirsutism (facial hair) and acne – androgenic hormones • Hypertension(80%) – mineralcorticoid effect • Elevated blood glucose (d/t enhanced glucogenesis and dec. glucose utilization ) • Muscle weakness (effect of gluco. on protein catabolism) • Suppressed immune system (loss protein in lymphoid tissue) • Osteoporosis – (d/t decreased protein deposition in bone)
Treatment of Cushing’s • Surgical removal of adrenal tumor, if this is cause • Surgical removal or radiation of hypertrophied pituitary gland • Drugs that block steroidgenesis • Otherwise, if ACTH secretion cannot be decreased by these means, only treatment is bilateral partial or total adrenalectomy, followed by administration of adrenal steroids