Download
1 / 41
420 likes | 755 Vues
Nicotine Replacement Therapy. Aims or NRT Nicotine kinetic Nicotine tools NRT use to start smoking cessation with hospitalised patients NRT Choice Dose adaptation Nicotine overdose symptoms Characteristics of withdrawal symptoms Cardiac and pregnancy Sleep problems

E N D
Nicotine Replacement Therapy Aims or NRT Nicotine kinetic Nicotine tools NRT use to start smoking cessation with hospitalised patients NRT Choice Dose adaptation Nicotine overdose symptoms Characteristics of withdrawal symptoms Cardiac and pregnancy Sleep problems Treatment duration Risk reduction
A turning point in smoking cessation history : Comfortable cessation, easier (compared with previous attempts). No longer contra-indicated for pregnant women or cardiac patients. Success percentage = placebo X 2. But still high relapse rate in the short term. Necessary improvements : dosage, follow up duration, relapse prevention… NRT Source : G. Lagrue
NRT initiated before entering the hospital should be continued on admission Cessation should be initiated to motivate dependant smokers For pregnant women in the maternity ward NRT can be used to avoid the withdrawal symptoms in heavy smokers hospitalised in casualty NRT use reduces the risks of tobacco related illnesses in dependant smokers Use of NRT for hospitalised patients :
Motivated smoker (step by step process) Personal decision Physically dependent smoker (Fagerström above 3) Immediate evaluation, taking behavioural and psychological dependence into account Condition for NRT efficiency (prior to quitting) Source : Conférence Consensus 1998
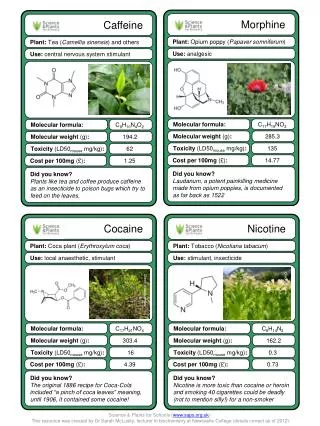
The nicotine quantity absorbed per day by a heavy smoker is variable : on average 30-40 mg for a heavy smoker that is to say around 1 mg per cigarette, but there are individual variations ++ : for 30 cig/d from 10 - 100 mg nicotine/day ! ! Each smoker maintains a regular level of nicotine in an automatic way by smoking cigarettes. In order to prevent withdrawal syndrome and the desire to smoke, nicotine has to be given in a satisfactory quantity, according to the nicotine intake which existed prior to cessation. Nicotine kinetic Source : G Lagrue
From Russel Nicotine Kinetic Nicotine plasmatic ng/ml 25 0 Cigarette Nasal Spray Gum 4 mg Patch 21 mg Inhalor Gum 2 mg 0 30 60 minutes
Smoking cessation is easy (less difficult) with the right tools: • Gum (2 mg – 4 mg : success 40 %) - Doubles success (20 to 40 % ) at the end of the treatment compared to placebo (10- 20 % according to associated psychological support) - Important behavioural component - Pros : the patient is an “actor” throughout the day. - Cons : buccopharyngeas troubles, if misused, dental apparatus, insufficient dosage (use 4 mg) • Sub-lingual tabs (Microtab 2 mg..) Similar to gum but without chewing, no hiccups • Patch - Nicotine delivered continuously at significant doses (5 to 21 mg) - Dosage easy to determine - Results 20-60% subjects abstinent at the end of the treatment (2-3 months) -Difficulties : continuous deliverance, therefore difficulties in facing unpredicted emotional shock • Inhaler NRT tools
Nicotine delivery: variations from one smoker to another according to: - number of gums chewed - ways of chewing the gums With the same number of gums, the nicotine level varies from 1 to 5 according to the subject. The 2 mg gum gives the required nicotine level to moderately dependant smokers (0,86 mg of nicotine delivered per gum). The 4 mg gum, if properly taken, delivers nicotine in doses close to patch (1,4 mg nicotine delivered per gum). The initial nicotine intake takes about 15 chews; when a tickle appears, place the gum between cheeks and teeth or gums; when the tickling disappears, start chewing again; each gum has to be chewed from time to time for 20 to 30 minutes. Gum
Advice on the use of Nicotine Gum • Nicotine Gum should be available for patient use on request. • The smoker needs to: • Be encouraged to take the necessary quantity to reduce the withdrawal symptoms. • Place the gum in the mouth and chew it slowly, taking the same length of time it would take to smoke a cigarette. Usually the gum lasts for at least 30 min. • Be taught to throw away used gum in a safe place in order to avoid a child using it (it contains residual nicotine). • Note the amount of gum used in order to monitor and adapt nicotine dosage. • Without over-dramatising, discourage smoking during this treatment.
Nicotine delivery: small variations from one subject to the other (maximum 1 to 2, against 1 to 10 for cigarettes). - Placement needs to be changed every day - Open wrapping with scissors - Secure the patchby applying the adhesive - Perspiration can un-stick the patch. There are a variety of patches: 16 hours/24 and patches 24/24 hours ( 10, 20 and 30 cm2). After the patch is removed, nicotine remains for 4 to 8 hours. Patch
Advice on the use of Patches • These transdermal devices must be applied on a clean and dry skin in the morning, replacing immediately the one from the day before (patch 24 hours) or replacing the one taken off before sleeping (patch 16 hours). • Its patch size (30, 20 or 10 cm2) determines the nicotine dosage. • Its position must be changed every day. • Use scissors to take the patch out of its packaging. • Avoid touching the adhesive part of the patch. • Avoid moistening the patch too long even if it resists water. • If the patch un-sticks it can be re-stuck. • After use, the patch is folded and put in a safe place in order to avoid children playing with it (significant dose of residual nicotine). • Without over-dramatising, discourage smoking during this treatment.
Results ”nicotine-patches"(treatment 2 to 3 months – 11 studies) doses 14-21 mg of nicotine • Results end of • treatment = 2339 • Results at 6 months • 7 studies n = 2044 • Percentage of relapse • Real patch • (success) • nbre % • 919 53 % • 265 26 % • 51 % • False patch • (success) • nbre % • 24 % • 12 % • 50 %
Optimise patch dosage(treatment 3 months) % abstinents 100 90 80 70 60 50 40 15mg 25mg 30 20 10 False patch 0 0 6 9 18 24 30 36 42 48 54 sem Source : Tonnenesen NEJM 99
Comparison of 3 NRT forms Results at 6 months – meta-analysis (50 studies) n =7834 (duration of treatment 2-3 months) Gum Patch Nasal spray All studies Active 18,2% 20,5% 20,0% 18,6% False 10,6% 10,8% 7,0% 10,6 % Relative abstinence level 1,61 2,07 2,9 1,71 C. Silagy – Lancet 15.01.94
NRT Indications for hospitalised patients Whatever the reason for being in hospital, cessation can be initiated, especially if the hospital stay is for several days. Life changes, smoke-free environment, psychological help for hospital staff are all favourable elements. If the smoker is dependant NRT is recommended. NRT dose can be determine by cotinine level, or based on smoking history and dependence
Advice for hospitalised patients ready to quit • Get the patient to decide to set their admission date as a quitting date. • Make the patient state precisely why they want to stop. • Enumerate obstacles to cessation. • Implement a plan to avoid temptations. • Advise the patient to seek help from family and friends. Source : American Lung Association
NRT Indications for smoking hospital patient (1) Being a hospital patient is an indication for NRT whatever stage of change (cessation) the dependant patient is at and whatever illness justifies his presence in the hospital. Substitution spares the patient suffering from severe withdrawal symptoms.
NRT prevents the smoking hospital patient smoke cigarettes in dangerous conditions (>40% fire starts in the hospital are cigarette related (AP-HP99). NRT can help the patient to realise that he is dependant on a substance (nicotine) and that NRT prevents withdrawal symptoms. This positive experience may facilitate a decision to stop smoking. NRT Indications for smoking hospital patient (2)
Psycho-behavioural dependence Neuro-pharmacological dependence Search for satisfaction via a specific nicotine dosage in blood NicotineReplacement TherapyNicotine Dependence The vast majority of cigarettes are not smoked out of pleasure but out of dependence: smoking is addictive: smoking on a regular basis is an illness like alcoholism.
Total smoking cessation. Sufficient initial dosage. Training for gum and patch use. Dosage adaptation. Follow up (to be organised when leaving the hospital). Relapse prevention. NRT efficiency requirements (during cessation) Source : Conférence Consensus 1998
Amongst the 3 NRT forms, choose the most adaptable Gum Patch Sublingual tabs Little dependence = 2 mg big dependence = 4 mg Oral and behavioural elements The smoker is active. He chooses his moments. Good option in the case of emergency. Advantages Average and high dependence Discrete Removes nicotine level peaks No dependence risks Pharmaco Kinetic close to gums Oral and behavioural elements The smoker is active. He chooses his moments. Less hiccup ups than with gums and Indications Under or over dose risk with no rapid adaptation No more activity required Under dosage risk (2mg). Use sometimes difficult: chewing problems. Some dependence cases (mainly with 4 mg). Chewing obvious to others Disadvantages Under dose risk Initial dose can be modulated according to response at 24 or 48 hours. Doses decrease 6 to 12 weeks. Continuous adaptation by the smoker, an average of 8-12 tabs/d. Continuous adaptation by the smoker, an average of 8-12 gums/d. Dosage Source: G. Lagrue
It is necessary to give the right nicotine quantity: - in order to remove the craving and withdrawal syndrome, - but avoid excess in order to prevent over dose. The initial evaluation of the nicotine should be precise: - the precise number of cigarettes smoked. The Fagerström test is more useful. - allows for greater individual variations. There is no biological test that can be used in order to determine the dose. Initiallygive the biggest patch if 20 cig or more withFagerström 5 or more. This dose can be reviewed upwards if withdrawal symptoms. Consider dose adaptation on the second day. Difficulties in adapting initial nicotine dosage
NRT use to start smoking cessation for hospitalised patients • Examples of proposed initial dosage (Dosages are best adapted based on the Fagerström test) 10-19 cig/day 20-30cig/day > 30 cig/day Smokes nothing or gum not every day not in the morning nothing or gum gum high dose patch High dose patch ± < 60' after high dose patch gum gum waking up high dose patch + gum < 30' after high dose patch ± high dose patch gum waking up < 5' after high dose patch ± high dose patch + high + medium patch ± gum gum waking up gum
Availability for nicotine gums to the necessary and sufficient daily dosage (6 to 16 gums/ day). Advice and information on how to take NRT and the daily dosage stated. Patches : easier to use, delivers a stable dose of nicotine. They make nicotine peaks disappear (doses can be adapted on day 2-3 if necessary). NRT for a dependent smoker in hospital
The dose has to be re-evaluated on the second day. A need to smoke despite NRT can lead to its increase. Oral forms of NRT are well designed for dose adaptation. A sufficient dosage is associated with the disappearance of the smoking urge. If within the hospital there is a mobile smoking cessation service, the nurse or cessation facilitator can visit patients and their relatives at ward/unit level. If there is only a smoking cessation counselling service, patients can be referred to this for a consultation. Indications to start NRT in hospital
They are rare. Always less important and less serious than smoking effects. Unjustified side effect fear must not lead to under dosage. However, have been seen : skin allergy due to patches, digestive trouble when gums are chewed to quickly, not as frequent with sublingual tabs (Microtab,..). Side-effects
Indications for nicotine replacement therapy for a hospitalised dependant smoker • The intake of oral forms together with patches allows a fast adaptation of transdermal doses (as for morphine). • Nicotine under dosage can lead the smoker to continue or resume smoking .
Nicotine overdose symptoms(less frequent than under dose) • No withdrawal symptoms, no desire to smoke • From the first day : • - Nausea, dizziness • - Palpitations, headaches • - Dry mouth (as if I had smoked too much) • - Severe insomnia • - Diarrhoea • Reduction of the doses disappearance of the symptoms
Nicotine overdose symptoms(less frequent than under dose) • No withdrawal symptoms, no desire to smoke. • From the first day : • - Nausea • - Palpitations, headaches • - Dry mouth (as if I had smoked too much) • - Severe insomnia • - Diarrhoea • Reduction of the doses disappearing of the symptoms
Dosage adjustment during the first week • If overdose signs... • Decrease dosage and/or no patch during the night. • If under dosage signs... • Increase nicotine substitute dosage, based on non-prescribed intake as well as on theinitial patch dose (cigarettes or 2 mg gums) and/or craving. • Very often dosage needs to be increased. • Establish over a few days, the dose that will eradicate the withdrawal syndrome and not show signs of overdose. • If smoking continues after 1 week, reassess the problem.
Indications for nicotine substitution in cardiovascular disease • Quitting smoking is vitally important • Coronary Heart Disease smoker: repeated vasoconstriction • High HbCO --> risk ++ • Myoglobine-CO • Immediate benefits from quitting: • - suppression of vasoconstrictor effect • - diminution of thromboses risk • - augmentation of blood fluidity • - better oxygenation • Nicotine replacement therapy is always less dangerous than smoking. • Nicotine replacement therapy - necessary when smoking persists • - safer than smoking +++
Risk reduction for pregnant women Cessation without NRT is best. Nicotine alone is better than smoking cigarettes : hundreds of toxic products are contained in tobacco smoke especially CO which can asphyxiate the baby. Nicotine in amniotic fluid : use preferably a treatment which lasts less than 24 hours : gum or 16 hour patch.
Cessation without NRT (or NRT under dose) - insomnia either when falling asleep (anxiety) or when awakening - duration from 2 to 4 weeks - tiredness when waking up - day time : lack of energy, sleepiness Cessation with NRT - insomnia with frequent awakenings - sleep length shortened, frequent dreams -If these are intense, take patch out when going to bed. Cessation with nicotine overdose - insomnia +++, shortening of sleeping duration, dreams+++ - good awakening, diurnal hyperactivity - troubles directly linked with nicotine: disappear when removing the patch in the evening. Rise of a depressive syndrome after cessation - insomnia, awakenings at night with ruminations - Intense tiredness when waking up, frequent nightmares - day time sleepiness Sleeping problems and smoking cessation Source: G. Lagrue
Very frequent, with very precise memories. Facilitated by nicotine patch, which brings more nicotine at night than a cigarette (you do not smoke while sleeping ! ! ) - With or without sleeping difficulties - Sometimes nightmare when waking up in this case suspicion of depression or anxious state. Dreams under NRT
Traditionally: 2-3 months -- doses decreasing 1 2 3 every 4 weeks (no long-term prescription without follow up). This can can be changed according to circumstances: • Sometimes shortened: no withdrawal symptoms despite omission. • Often has to be continued after three months: - Reappearance of the craving - Anxiety (problems) - Temptation: environment NRT duration Source : G Lagrue
Nicotine for risk reduction • Risk reduction for a smoking related • illness • Risk reduction cardiovascular disease • Risk reduction for respiratory illness • Risk reduction for pregnant women • Risk reduction prior to surgery
Risk reduction for a smoking related illness • NRT is prescribed for hospital patients affected by a smoking related illness even without a voluntary request. • It enables a consumption decrease (not compensated by a change in smoking habits) : • for cardiac patients • for respiratory patients • for pregnant women • before surgical operation
For all coronary related illness, NRT is better than smoking. NRT brings no CO, no irritants, which play a leading role in the onset of cardiac incidents. For patients with severe coronary condition, total absence from nicotine intake is targeted. (If the smoker cannot do without nicotine, NRT is better than smoking.) NRT can be prescribed very soon after a myocardial infarction. Risk reduction for cardiovascular disease
Risk reduction for respiratory illness • NRT has no respiratory effect. • In less than 24 hours cough diminishes. • NRT diminishes symptoms before an endoscopy, even if the patient is not willing to quit smoking.
Risk reduction for pregnant women Cessation without NRT is better. Nicotine alone is better than smoking cigarette : hundreds of toxic products are contained in tobacco smoke especially CO which can asphyxiate the baby. Nicotine in amniotic fluid : use preferably a treatment which lasts less than 24 hours : gum or 16 hours patch.
Smoking cessation prior to having surgery: ameliorates anaesthesia conditions (necessary doses are less important, easier wakening, cough less important) reduces the risk of infection, helps healing. Risk reduction prior to surgery