Understanding Giardia: A Comprehensive Overview of Infection, Symptoms, and Treatment
430 likes | 635 Vues
Giardia intestinalis, a flagellate protozoan, is a worldwide cause of gastrointestinal illness, primarily transmitted through contaminated water and food. This organism exists in two forms: trophozoites and cysts. Symptoms of infection can range from asymptomatic to severe diarrhea, abdominal pain, and malabsorption syndromes, especially in young or immunocompromised individuals. Diagnosis involves stool examination and serological tests. Treatment options include Metronidazole and Albendazole. Preventive measures focus on environmental hygiene and safe food practices.

Understanding Giardia: A Comprehensive Overview of Infection, Symptoms, and Treatment
E N D
Presentation Transcript
A- Oro-intestinal- urogenital flagellates: General Characters: 1- Infection occurs in the buccal cavity, the intestine or the uro-genital tract. 2- The infective stage is either the vegetative or the cystic form. 3- Transmission of infection is direct one.
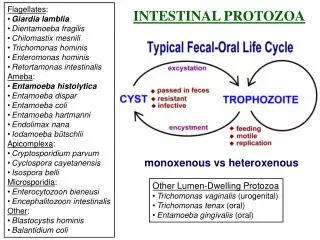
1- Giardia intestinalis(Giardia lamblia) Geographical distribution: world-wide. It is considered the main cause of diarrheal outbreaks from contaminated water supplies. Morphology: Tow forms can be visualized microscopically. A- Trophozoite B- Cyst
A- Trophozoite: • The body is bilaterally symmetrical. • Size: 12 x 6 μ. • It is pear-shaped with an anterior rounded and posterior tapering parts. • It has a convex dorsal surface and a flat ventral one which is modified in its anterior part forming a sucking disk acting as an attachment organ.
Trophozoite: • Two vesicular nucleus. • Two median bodies (curved rods) called parabasal bodies. - Four pairs of flagella. -The intracytoplasmic part (axonemes) of posterior two flagellae (axostyle) extend through the body dividing it and become free posteriorly.
B- Cyst: - Size is 10 x 5 μ. • It has double-colourless wall. • It contains four nuclei usually gathered at one pole. • Cytoplasm is often retracted at one side. • Remnants of the flagellae, median bodies and axostyle are clearly seen.
Life Cycle: Habitat:-In the upper part of small intestine (duodenum and upper jejunum). - Trophozoites stick closely to the mucosa and they may penetrate the crypts of mucosa. • They may be found in the gall bladder and bile ducts. Definitive host:Man is the natural host. Reservoir hosts: Many animals (dogs, rodents, monkeys, pigs….ect.) Giardia is a zoonotic disease. Infective stage:Maturequadrinucleated cyst.
Mode of infection: faeco-oral transmission cycle: 1) Cysts may be ingested with contaminated food and water or transmitted by house flies, cockroaches…ect. 2) Person to person transmission occurs especially among school children, prisoners and in nurseries. 3) Autoinfection by hand-to-mouth transmission. • Trophozoites replicate by longitudinal binary fission. • Excystation occurs in upper part of the small intestine stimulated by alkaline pH there. • Cyst → two trophozoites.
Pathogenecity and Clinical Picture: • Trophozoites live closely to intestinal mucosa attached by their sucking discs→ mechanical irritation. • Attachment is facilitated by a parasite secreted lectin which is activated by duodenal secretion→ derangement of normal villous architecture. • Shortening, blunting of villi up to total atrophy. • Inflammatory foci in crypts and lamina propria.
Resistance to giardiasis: It is indicated by spontaneous cure of the disease that may occur after about 40 days. • Lymphocytes, macrophages and secretory IgA are important for resistance. • Human Milk is able to kill Giardia trophozoites via lipase and IgA, so it can afford protection to breast fed babies. The prepatant period is 10-36 days. The disease may be asymptomatic in many cases.
Symptoms may be: 1) Diarrhea, flatulance, distension, epigastric pain, crampy abdominal pain, anorexia and weight loss.
2) Sreatorrhea (fatty diarrhea) and malabsorption syndrome (Steatorrhea → greasy, pale yellow, frothy foul smelling and bulky stool) may occur due to: a- Physical occlusion of mucosa by attached parasites. b- Enterotoxin secretions by the parasite. c- Deconjugation and consumption of the bile salts. d- Villous atrophy. This patient has: - ↓absorption of carotene, folate and vit B12 • ↓ activity of lipase, ↓ secretion of disaccharidases, lactose and other enzymes → Lactose intolerance.
3) Severe symptoms: (in immunocompromized) • Persistent steatorrhea. • Fat-soluble vitamins deficiency. • Hypoproteinaemia • Cholangitis and cholecystitis → jaundice & biliary colic Predisposing factors to symptomatic giardiasis: 1- Achlorohydria, hypogammaglobinaemia and relative ↓ secretory IgE. 2- Young age (infants and children). 3- Bacterial colonization ↑ damage by Giardiatrophozoites.
Diagnosis: • Clinical diagnosis: C/P of the disease. • Laboratory diagnosis: A- Direct: - Stool examination by direct smear- concentration methods. ** Repeated ex. for 3 times must be done (due to intermittent shedding of the parasite). - Examination of duodenal fluid which may be taken by duodenal aspiration or by Enterotest (string-test). B- Indirect: - Serological tests: IFA and ELISA. - Detection of copro-antigen by ELISA.
Treatment: • Fasigyn as a single dose. • Metronidazole (Flagyl). (Not given to pregnant women: teratogenic) 3) Albendazole. Prevention and Control: - Environmental sanitation as: anti-fly measures, proper sewage disposal and safe water supply. - Faeces must not be used as fertilizer. - Health education for: washing of green vegetables, fruits and hands before eating. - Treatment of cases especially the carriers.
The Non-Pathogenic Intestinal Flagellates All inhabit large intestine. All are harmless commensals. Multiplies by binary fission. The cyst is the infective stage. 1- Embadomonas (Retortamonas) intestinalis Trophozoite: elongate, pyriform, 6×4μ in size. - Anterior cleft-like cytostome. - One vesicular nucleus. - Two blepharoplasts give rise to 2 flagellae (one directed anteriorly & the other pass through cytostome posteriorly free. Cyst: uninucleated, pyriform, 5×4μ in size.
2- Chilomastix mesnili Trophozoite: asymmetrical pear shaped, about 15×8μ in size. - Anterior cleft-like cytostome. - One vesicular nucleus. - Six blepharoplasts (near nucleus) give rise to 3 free flagellae anteriorly, 2 surround the margins of the cytostome & the last pass through it. Cyst: uninucleated, lemon-shaped, 6×8μ in size.
Chilomastix mesnili Trophozoite: Cyst:
3- Enteromonas hominis Trophozoite: oval in shaped, about 16×4μ in size. - No cytostome. - One vesicular nucleus. - Four blepharoplasts (near nucleus) give rise to 3 free flagellae anteriorly, & the fourth pass posteriorly. Cyst: ovoidal in shaped, 5×4μ in size. Mature cyst is quadrinucleated.
Human Trichomonads There are 3 species: 1-Trichomonus vaginalis. 1-Trichomonus hominis (intestinalis). 2-Trichomonus tenax (buccalis). -They have 4 anterior flagellae, an undulating membrane, an axostyle and a cytostome. - There is no cyst formation but exist only in the trophozoite stage (The infective stage).
Trichomonas vaginalis (Pathogenic urogenital flagellates) Disease:Trichomoniasis, trichomonad vaginitis, urethritis, prostate vesiculitis. Geographical distribution: world wide. Morphology: - It is colourless pyriform flagellate (robust) - Size is 17 × 10 μ, • Anterior cleft-like cytostome. • One vesicular nucleus. • Four flagellae directed anteriorly, • Another one attach to 1/3 of the body of the parasite undulating membrane. • The 6th flagellum passes through the body as thin axostyle and projects out posteriorly. - A thick rod called parabasal body present between axostyle and the undulating membrane.
F U A 10 mm Trichomonas vaginalis trophozoite
Life cycle: • Habitat: -In females: posterior fornix of the vagina, cervix and sometimes urethra -In males: urethra, epididymis, prostate & seminal vesicles. • Definitive host:only man (no intermediate host). • Infective stage:trophozoites. • Mode of infection: 1- Transmission occur during sexual acts or through contaminated inner clothes, towels, toilet seats…ect. 2- Trichomonas conjunctivitis may affect babies that acquired the infection while passing through the birth canal of their infected mothers. • Multiplication: by longitudinal binary fission.
Pathogenesis & Clinical picture: • Up to 50% of infected females & 95% of infected males are asymptomatic. • The parasite is able to produce contact dependent cytopathic effect (kill cells without phagocytosis). • Also it produces a cell detaching factor (its amount correlates with severity of the manifestation). Predisposing factors for pathogenicity: - Change of normal acidic vaginal pH: 3.8- 4.4 (due to lactic acids produced by Doderlein’s bacilli bacterial flora) in to alkaline side (↑ pH). - Change of physiologic status of the vagina and ↓ the secretory IgA.
1) In Female: - In Trichomonas vaginitis, vaginal walls are red, tender with hyperaemia and petechial haemorrhage. • Mucosa shows erosion and necrosis • Vaginal surface is covered by seropurulent, frothy creamy or yellowish exudates. • Patients complaint of: - Itching and burning sensation with profuse yellowish leucorrheic discharge. - Dyspareunia (painful sexual intercourse), dysuria and frequency of micturation can occur, also cystitis. ( A relation to cervical carcinoma was suggested).
2) In Males: • Infection generally is asymptomatic but urethritis vesiculitis, epididymitis and prostatitis may occur. • Patients complaint of: - Dysuria with thin discharge. - Enlarged prostate with tender epididymis. 3) In New born: - Trichomonas respiratory tract infection and conjunctivitis may occur.
Diagnosis: • Clinical diagnosis: C/P of the disease. • Laboratory diagnosis: A- Demonstration of the trophozoite. In females: - specimens obtained via vaginal speculum. In males: - examination of prostatic fluid. - Direct wet smear examination by phase-contrast microscope ( motile trophozoites). - Staining with Giemsa, Leishman or Papanicolaou stains. - Examination of urine and urethral discharge in both. B- Culture of specimens on Modified Diamond media. C- Immunological tests for detection of T. vaginalis antigens in the discharge by: - Direct fluorescent test using labeled monoclonal antibodies(DFA). - Enzyme immunoassay.
Treatment: 1- Both partners must be treated at the same time. 2- Local vaginal suppositories as Silver picrate and Furazolidone. 3- Vaginal douching with lactic acid or vinegar for restoration of normal vaginal pH. 4- Metronidazole (most effective) It is used after failure of local measures (?carcinogenic). Prevention and control: • Attention to personal hygiene and health education. • Treatment of cases. • Abstinence from using common toilet articles.
Two other species of Trichomonas occur in humans Pentatrichomonas hominis
Trichomonas hominis (T. intestinalis) It is non pathogenic & inhabit the large intestine. - Small, 12x8μ, pyriform. - Has small antero-lateral cytostome (mouth), one nucleus, four free flagella anteriorly and one marginal forming undulating membrane along 2/3 length of the parasite with free end. - Thick axostyle (flagellum) extends antro-posteriorly along the middle of the body, with no parabasal body. -Transmission is direct, through contaminated food and drink by the vegetative form.
Trichomonas tenax(T. buccalis) - It is non pathogenic parasite that inhabits the mouth especially in carious teeth & gums. - It measures 10x6μ , pyriform in shape. - Has cytostome, one nucleus, 4 free flagella and one marginal with undulating membrane 1/2 the lateral margin of the parasite with no free end. - Slender axostyle and faint parabasal body. - Transmission is by the use of contaminated utensils with the trophozoite or direct by kissing.
Dientamoeba fragilis It was considered to be an amoeba, but its flagellate nature was discovered by electron microscope. It is now classified among the trichomonads. Geographical distribution: world wide. Morphology: - It has no cyst stage. • Trophozoite: 7 × 12 μ, characterized by the presence of two nuclei. • Their karyosomes are composed of granules 4-8 in number. • Cytoplasm contains food vacuoles (contain bacteria). • Pseudopodia are leaf-like active in fresh stool.
Habitat:mucosal crypts of large intestine of man. (It may ingest RBCs but never invades the mucosa). Infective stage: trophozoite. Mode of transmission: Transmission might occur via eggs of Entrobius vermicularis or Ascaris (trophozoite inside the egg) as oral transmission failed. Clinical picture: mucus diarrhea, abdominal pain, flatulence and weakness. Diagnosis: careful examination of fresh saline smear of stool. Staining with iron haematoxylin is preferable. Treatment: - Idioquinol - Tetracycline - Paromomycin