Download
1 / 1
10 likes | 162 Vues
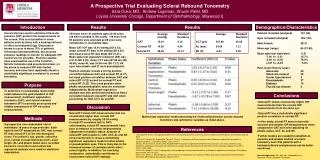
A Prospective Trial Comparing Pneumotonometry of Cornea and Sclera. Usiwoma Abugo BS 1 , Sara Duke MD 2 , Shuchi Patel, MD 2 1 Loyola University Chicago, Stritch School of Medicine, Maywood IL 2 Department of Ophthalmology, Loyola Medicine, Stritch School of Medicine, Maywood, IL. ABSTRACT

E N D
A Prospective Trial Comparing Pneumotonometry of Cornea and Sclera Usiwoma Abugo BS1 ,Sara Duke MD2 ,Shuchi Patel, MD2 1Loyola University Chicago, Stritch School of Medicine, Maywood IL 2Department of Ophthalmology, Loyola Medicine, Stritch School of Medicine, Maywood, IL ABSTRACT Purpose: Current devices in use to estimate intraocular pressure (IOP) perform the measurements on the cornea. However this is not practical or possible in some patients, such as those with a keratoprosthesis or other corneal pathology. Therefore scleral IOP measurements have been attempted but studies have shown that the Tonopen does not provide accurate readings with scleral measurements. The purpose of this study is to determine if scleral pneumotonometry (PT) will provide an accurate and reliable assessment of IOP. Also, if scleral tonometry is not accurate but is reliable, perhaps a predictable relationship exists and thus IOP can be extrapolated from scleral measurement. Methods: A prospective non-randomized trial of individuals 18 years of age and older. Each had his/her IOP measured with the Goldmann applanation tonometer (GAT) as the gold standard. Then corneal PT and scleral PT on the temporal sclera were performed. Results: 108 eyes have been examined to date. The average GAT IOP was found to be 15.03 mmHg while the average corneal PT was 18.5 mmHg. The difference between GAT and corneal PT measurements was 3.4 with a mode of the differences at 2.0 and 57 of the 108 eyes being over 3 mmHg higher with corneal PT. The average scleral PT was 29.4 with an average difference between GAT and scleral PT measurements of 14.3 and a mode of 14 with 53 of the 108 eyes above 15 mmHg higher with scleral PT. Conclusion: Thus far scleral PT has shown consistently higher IOP measurements than the corneal IOP measurements in the majority of patients. Yet, there seems to be a predictable correlation with the IOP being 14 points higher when measured on the sclera as compared to the gold standard. With further data collection and analysis we anticipate that a predictable relationship, that may or may not be linear, between scleral PT and both corneal PT and GAT can be established. RESULTS The average GAT IOP was found to be 15.0mmHg while the average corneal PT was 18.5mmHg. The difference between GAT and corneal PT measurements was 3.4mmHg with a mode of the differences at 2.0mmHg and 57 of the 108 eyes being over 3mmHg higher with corneal PT. The average scleral PT was 29.4mmHg with an average difference between GAT and scleral PT measurements of 14.3mmHg and a mode of 14mmHg with 53 of the 108 eyes above 15mmHg higher with scleral PT. MATERIALS AND METHODS RESULTS This was a prospective non-randomized trial evaluating the accuracy and reliability of scleral PT. The study was performed at the ophthalmology clinic of the Loyola Hospital Outpatient Center, Maywood IL. Patients were recruited and consented in clinic by a member of the investigative team. Patients were selected based on the following inclusion criteria: >18 years of age, male or female, ability to understand study procedures and to comply with them for the entire length of the study. Patients were excluded if they were <18 years of age, had unwillingness or inability of individual or legal guardian/representative to give written informed consent. Patient’s demographic information (age, gender), ocular history, refractive error, current medications, PT, GAT and central corneal thickness readings were collected. Adherence was defined as at least 80% participation in tonometry measurements at the study visit. Values from patients who did not meet the adherence guideline were not included in the analysis of the study results. At the initial visit IOP measurements from both eyes were obtained. The first measurement was taken on the central cornea with a Goldmann Applanation Tonometer AT 900®D (Haag-Streit International). Then corneal IOP was measured with a Model 30 Classic Pneumatonometer (Reichert Ophthalmic Instruments). Scleral IOP was measured 2mm temporally from the limbus. Corneal Pachymeter was then measured with the DGH Model 555 PACHETTE 3(DGH Technology Inc.). DISCUSSION • In our study scleral PT was consistently higher than GAT or corneal PT for the majority of the patients in the study. • Of the 13 patients whose scleral PT was lower there was no unique eye pathology distinguishing those eyes from the rest of the population. • Even with the consistent elevation in scleral IOP preliminary analysis shows great variability in measurements obtained with the pneumatonometer. • This observation itself does not rule out the use for scleral pneumotonometry in the future but points to the need for elimination of variability in the instrument itself or the measurement taking. Comparison of Average GAT-C(mmHg), PT-C(mmHg), PT-Scl(mmHg). GAT-C was found to be 15.0mmHg ± 3.3mmHg. PT-C was found to be 18.5mmHg ± 3.9mmHg. PT-Scl was found to be 29.4mmHg ± 9.4mmHg. FUTURE DIRECTIONS Further studies analyzing other factors that may affect the relationship between GAT and scleral PT such as pachymetry and age should be conducted to better establish such a relationship and to eliminate some of the variability. In the future a conversion table may be established to provide better IOP readings in patients that cannot have corneal tonometry and are being monitored with finger tonometry alone. REFERENCES http://www.calcoastophthalmic.com/images/reichert_pneuma.jpg Comparison of the Differences between pneumotonometry of the Sclera and Applanation(PTC-TA), pneumotonometry of the Sclera and Applanation(PTS-TA), and pneumotonometry of the Sclera and pneumotonometry of the Cornea(PTS-PTC). PTC-TA was found to be 3.379 ±2.301mmHg. PTS-TA was found to be 14.3 ± 9.4mmHg. PTS-PTC was found to be 10.6 ± 9.2mmHg. • Barraza RA, Sit AJ. Investigation to determine a relationship between scleral and corneal tonometry. ARVO poster presentation; May 02, 2010. • Eisenberg DL, Sherman BG, McKeown CA, Schuman JS. Tonometery in adults and children: a manometric evaluation of pneumotonometry, applanation and TonoPen in vitro and in vivo. Ophthalmology: vol 105; 1173-1181. • Erlich JR, Haseltine S, Shimmyo M, Radcliffe NM. Evaluation of agreements between intraocular pressure measurements using GAT and Goldmann correlated intraocular pressure by Reichert’s ocular response analyzer. Eye: 2010; 1555-1560. • Shen CC, Downs J, Mansberger SL. Assessment of intraocular pressure along the limbus and sclera using contact and indentation tonometry. ARVO poster presentation; May 02, • ACKNOWLEDGEMENTS: • This work was supported by The Richard A. Perritt Charitable Foundation and The Illinois Society for the Prevention of Blindness. http://pages.glaucoma-association.com/cache/cfx_imagecr3/5381dc677c652311eb5d0d4663eed09b.jpg http://accessmedicine.net/loadBinary.aspx?name=tint&filename=tint_c636f028t.jpg