Download

1 / 68
680 likes | 687 Vues
Learn about swing bed services and hospital management solutions offered by Gaffey Healthcare and HealthTechS3. Get expert insights and strategies for continuous survey readiness.

E N D
5110MarylandWay,Suite200,Brentwood, TN 2745NorthDallasPkwy,Suite100,Dallas, TX 800.228.0647 www.gaffeythealthcare.com 615.309.6053 www.healthtechs3.com Swing Bed 101 September 6, 2019
Nationwide ClientBase • Currently provides hospital management, consulting services and technologyto: • Serving community, district,non-profit Preferred vendorto: • California Critical Access Hospital Network • Western HealthcareAlliance • Partner with Illinois Critical Access HospitalNetwork • Vizient Group PurchasingOrganization and critical accesshospitals • Example managed hospital client includes• Barrett Hospital and Healthcare inDillon, • MT. Ranked as a Top 100 Critical Access Hospital for 8 years in arow • Example technology and ARservices • client includes two-hospital NFP system in southeast GA with numerous associated physicianpractices
Areas ofExpertise Strategy–Solutions-Support Governance &Strategy Finance • Performance optimization & marginimprovement • Revenue cycle & business officeimprovement • ARoutsourcing • Executive management & leadershipdevelopment • Community health needsassessment • Leanculture Recruitment Clinical Care &Operations • Executive and interimrecruitment • CEOs, CFOs,CNOs • VP and DepartmentDirectors • Continuous surveyreadiness • Carecoordination • Swing bedconsulting
PRESENTER Carolyn began her healthcare career as a staff nurse in Intensive Care. She has worked in a variety of staff, administrative and consulting roles and has been in her current position as Regional Chief Clinical Officer with HealthTechS3 for the last fifteenyears. In her role as Regional Chief Clinical Officer,Carolyn St.Charles conducts mock surveys for Critical Access Hospitals, Acute Care Hospitals, Long Term Care, Rural Health Clinics, Home Health and Hospice. Carolyn also provides assistance in developing strategies for continuous survey readiness and developing plans of correction. Carolyn St.Charles Regional Chief ClinicalOfficer Carolynhas extensive experience in working with rural hospitals to both develop and strengthen SwingBed programs. carolyn.stcharles@healthtechs3.com 360-584-9868
INSTRUCTIONS FOR TODAY’SWEBINAR You may type a question in the text box if you have a question during thepresentation We will try to cover all of your questions – but if we don’t getto them during the webinar we will follow-up with you bye-mail You may also send questions after the webinar to our team (contact information is included at the end of thepresentation) www.healthtechs3.com The webinar will be recorded and the recording will be available on the HealthTechS3 web site: www.healthtechs3.com HealthTechS3 hopes that the information contained herein will be informative and helpful on industry topics. However, please note that this information is not intended to be definitive. HealthTechS3 and its affiliates expressly disclaim any and all liability, whatsoever, for any such information and for any use made thereof. HealthTechS3 does not and shall not have any authority to develop substantive billing or coding policies for any hospital, clinic or their respective personnel, and any such final responsibility remains exclusively with the hospital, clinic or their respective personnel. HealthTechS3 recommends that hospitals, clinics, their respective personnel, and all other third party recipients of this information consult original source materials and qualified healthcare regulatory counsel for specific guidance in healthcare reimbursement and regulatory matters.
3rdQUARTER 2019WEBINARS ALL WEBINARS ARE RECORDED Understanding the ROI on Advanced Wellness Visits and Advanced Care Planning: Preparing the Right Person for the Job Host: Faith M Jones, MSN, RN, NEA-BC – Director of Care Coordination and Lean Consulting, HealthTechS3July 11, 2019 at 12:00 pm CT https://bit.ly/2Xs2YUN Using the Concepts of Lean to Improve Swing Bed DocumentationHost: Carolyn St.Charles, RN, BSN, MBA – Chief Regional Clinical Officer, HealthTechS3July 12, 2019 at 12:00 pm CThttps://bit.ly/2Ju7JmU Community Health Needs Assessment – The Implementation PlanHost: Carolyn St.Charles, RN, BSN, MBA – Chief Regional Clinical Officer, HealthTechS3August 2, 2019 at 12:00 pm CT https://bit.ly/2xzek9U Improve your CCM Program Revenue: Incorporate Technology and Resources for Additional ReimbursementHost: Faith M Jones, MSN, RN, NEA-BC – Director of Care Coordination and Lean Consulting, HealthTechS3 August 15, 2019 at 12:00 pm CT https://bit.ly/2S08gAC Swing Bed 101Host: Carolyn St.Charles, RN, BSN, MBA – Chief Regional Clinical Officer, HealthTechS3September 6, 2019 at 12:00 pm CT https://bit.ly/2xHt8Dj Trends Facing Rural Healthcare BoardsHost: Michael Lieb – Regional Vice President & Director, Practice Management, HealthTechS3September 13, 2019 at 12:00 pm CT https://bit.ly/2YJVSaA
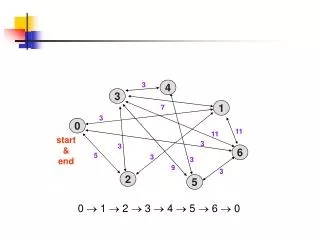
July 27,2018 1,350CAHs 1,183 provide Swing Bedservices
Use of Swing Beds IS NOT restricted to Medicare and Medicaid patients – just like admission to acute care is not restricted to only Medicare or Medicaid (Reimbursement may be different – of course)
REGULATORYRESOURCES • State Operations Manual – Appendix A (Rev. 183, 10-12-18) • State Operations Manual - Appendix W (Rev. 183,10-12-18) • StateOperationsManual -AppendixPP (Rev. 173,11-22-17) • Medicare Claims Processing Manuals – Updated in 2019 • Medicare Claims Processing Manual, Chapter 4 (Rev. 4295, 5-03-19) • Medicare Claims Processing Manual, Chapter 6 (Rev. 4247, 03-01-19) • Medicare Benefit Policy Manual Chapter 8 (Rev. 4202, 01-18-19)
What is a Swing Bed? The Social Security Act (the Act) permits certain small, rural hospitals to enter into a swing bed agreement, under which the hospital can use its beds, as needed, to provide either acute or SNF care. As defined in the regulations, a swing bed hospital is a hospital or critical access hospital (CAH) participating in Medicare that has CMS approval to provide post-hospital SNF care and meets certain requirements. Medicare Part A (the hospital insurance program) covers post-hospital extended care services furnished in a swing bed hospital. https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/SNFPPS/SwingBed.html
What is a Swing Bed? • Payment • CAHs that offer swing bed services are exempt from SNF PPS. These CAHs are paid for their SNF-level services based on 101 percent of the reasonable cost of the services (Medicare patients). • PPS Hospitals with Swing Beds are paid a per-diem rate which is case-mix adjusted using a resident classification system (Resource Utilization Groups IV) based on data from resident assessments (MDS 3.0) and relative weights developed from staff time data. • Length of Stay • There is no length of stay restriction for swing-beds – HOWEVER, criteria for swing bed must be met! • Swing bed may be used even if a SNF bed is available in the community There is no Medicare requirement to place a swing-bed patient in a nursing home and there are no requirements for transfer agreements between CAHs and nursing homes
Payment Methodology Critical Access Hospitals: Cost Based Reimbursement (Medicare) Rural PPS Hospitals: RUG-IV (Resource Utilization Group) Rural PPS Hospitals: October 2019 - Patient Driven Payment Model (PDPM)
Rural Hospitals (PPS) with Swing BedPayment Driven Payment Model - PDPM What is PDPM? The Patient Driven Payment Model (PDPM) is a new case-mix classification system for classifying skilled nursing facility (SNF) patients in a Medicare Part A covered stay into payment groups under the SNF Prospective Payment System. Effective beginning October 1, 2019, PDPM will replace the current case-mix classification system, the Resource Utilization Group, Version IV (RUG-IV). Why is CMS changing from RUG-IV to PDPM? Under RUG-IV, most patients are classified into a therapy payment group, which uses primarily the volume of therapy services provided to the patient as the basis for payment classification. This creates an incentive for SNF providers to furnish therapy to SNF patients regardless of the patient’s unique characteristics, goals, or needs. PDPM eliminates this incentive and improves the overall accuracy and appropriateness of SNF payments by classifying patients into payment groups based on specific, data-driven patient characteristics, while simultaneously reducing administrative burden on SNF providers. How are SNF patients classified into payment groups under PDPM? The PDPM classification methodology utilizes a combination of six payment components to derive payment. Five of the components are case-mix adjusted to cover utilization of SNF resources that vary according to patient characteristics. There is also an additional non-case-mix adjusted component to address utilization of SNF resources that do not vary by patient. Different patient characteristics are used to determine a patient’s classification into a case-mix group (CMG) within each of the case-mix adjusted payment components. The payment for each component is calculated by multiplying the case-mix index (CMI) that corresponds to the patient’s CMG by the wage adjusted component base payment rate, then by the specific day in the variable per diem adjustment schedule when applicable. The payments for each component are then added together along with the non-case-mix component payment rate to create a patient's total SNF PPS per diem rate under the PDPM https://www.cms.gov/medicare/medicare-fee-for-service-payment/snfpps/pdpm.html#fact
Critical Access Hospitals ---- Important Information Too! What is PDPM? The Patient Driven Payment Model (PDPM) is a new case-mix classification system for classifying skilled nursing facility (SNF) patients in a Medicare Part A covered stay into payment groups under the SNF Prospective Payment System. Effective beginning October 1, 2019, PDPM will replace the current case-mix classification system, the Resource Utilization Group, Version IV (RUG-IV). Why is CMS changing from RUG-IV to PDPM? Under RUG-IV, most patients are classified into a therapy payment group, which uses primarily the volume of therapy services provided to the patient as the basis for payment classification. This creates an incentive for SNF providers to furnish therapy to SNF patients regardless of the patient’s unique characteristics, goals, or needs. PDPM eliminates this incentive and improves the overall accuracy and appropriateness of SNF payments by classifying patients into payment groups based on specific, data-driven patient characteristics, while simultaneously reducing administrative burden on SNF providers. How are SNF patients classified into payment groups under PDPM? The PDPM classification methodology utilizes a combination of six payment components to derive payment. Five of the components are case-mix adjusted to cover utilization of SNF resources that vary according to patient characteristics. There is also an additional non-case-mix adjusted component to address utilization of SNF resources that do not vary by patient. Different patient characteristics are used to determine a patient’s classification into a case-mix group (CMG) within each of the case-mix adjusted payment components. The payment for each component is calculated by multiplying the case-mix index (CMI) that corresponds to the patient’s CMG by the wage adjusted component base payment rate, then by the specific day in the variable per diem adjustment schedule when applicable. The payments for each component are then added together along with the non-case-mix component payment rate to create a patient's total SNF PPS per diem rate under the PDPM https://www.cms.gov/medicare/medicare-fee-for-service-payment/snfpps/pdpm.html#fact
Swing Bed Program Benefits • Critical Access Hospitals • Cost based reimbursement for Medicare • No delays in providing skilled level of care (no transfers • Rural PPS Hospitals • No delays in providing skilled level of care (no transfers) • May reduce acute care length of stay • Patients • Care close to home • Usually same provider(s), nursing staff, rehab staff • Usually a shorter length of stay than in a SNF
Swing Bed Program Challenges • Paperwork • Discharge from Acute • Admission to Swing Bed • Assessment (MDS for Rural PPS Hospitals) • Multidisciplinary Plan of Care • Discharge • SNF Level Care • Staff and Provider understanding of how and why swing bed is different than acute care – and providing SNF level care • Activities • Providing sufficient type and frequency of activities • Volume • Too many swing bed patients and concern about capacity for acute patients • Too few swing bed patients to ensure consistent and reliable processes
Medicare Swing Bed Criteria Private Insurance – TheirRules Medicaid – Different by State – TheirRules Medicare The patient has Medicare Part A and has benefit daysavailable Medicare age or disability/disease eligibility requirements must bemet There must be a three‐day qualifying stay (observation doesn’tcount) Swing Bed admission condition is the same as the qualifying staycondition Patient must be admitted to Swing Bed within thirty days of discharge from acutecare The patient’s condition meets criteria to necessitate inpatient skilled nursingservices Medicare Benefit Policy Manual Chapter 8 (Rev. 4202, 01-18-19) Coverage of Extended Care (SNF) Services Under HospitalInsurance
Medicare 3-day Qualifying Stay • The 3 consecutive calendar day stay requirement can be met by stays totaling 3 consecutive days in one or more hospitals. • In determining whether the requirement has been met, the day of admission, but not the day of discharge, is counted as a hospital inpatient day. • Time spent in observation status or in the emergency room prior to (or in lieu of) an inpatient admission to the hospital does not count toward the 3-day qualifying inpatient hospital stay, as a person who appears at a hospital’s emergency room seeking examination or treatment or is placed on observation has not been admitted to the hospital as an inpatient; instead, the person receives outpatient services. • Medicare Benefit Policy Manual Chapter 8 – 20.1
Medicare Qualifying Condition To be covered, the extended care services must have been for the treatment of a condition for which the beneficiary was receiving inpatient hospital services (including services of an emergency hospital) or a condition which arose while in the SNF for treatment of a condition for which the beneficiary was previously hospitalized. In this context, the applicable hospital condition need not have been the principal diagnosis that actually precipitated the beneficiary’s admission to the hospital, but could be any one of the conditions present during the qualifying hospital stay. Medicare Benefit Policy Manual Chapter 8 – 20.1
Medicare Daily Skilled Care 30.6 - Daily Skilled Services Defined (Rev. 249, Issued: 11-02-18, Effective: 12-04-18, Implementation: 12-04-18) Skilled nursing services or skilled rehabilitation services (or a combination of these services) must be needed and provided on a “daily basis,” i.e., on essentially a 7-days-a week basis. A patient whose inpatient stay is based solely on the need for skilled rehabilitation services would meet the “daily basis” requirement when they need and receive those services on at least 5 days a week. (If therapy services are provided less than 5 days a week, the “daily” requirement would not be met.) Coverage of nursing care and/or therapy to perform a maintenance program does not turn on the presence or absence of an individual’s potential for improvement from the nursing care and/or therapy, but rather on the beneficiary’s need for skilled care. Medicare Benefit Policy Manual Chapter 8 – 20.1
Daily Skilled Care • A patient who normally requires skilled rehabilitation services on a daily basis may exhibit extreme fatigue, which results in suspending therapy sessions for a day or two. Coverage may continue for these days since discharge in such a case would not be practical. • In instances when a patient requires a skilled restorative nursing program to positively affect his functional well-being, the expectation is that the program be rendered at least 6 days a week. (Note that when a patient’s skilled status is based on a restorative program, medical evidence must be documented to justify the services. In most instances, it is expected that a skilled restorative program will be, at most, only a few weeks in duration.) • The daily basis requirement can be met by furnishing a single type of skilled service every day, or by furnishing various types of skilled services on different days of the week that collectively add up to “daily” skilled services. However, arbitrarily staggering the timing of various therapy modalities through the week, merely in order to have some type of therapy session occur each day, would not satisfy the SNF coverage requirement for skilled care to be needed on a “daily basis.” To meet this requirement, the patient must actually need skilled rehabilitation services to be furnished on each of the days that the facility makes such services available. • It is not sufficient for the scheduling of therapy sessions to be arranged so that some therapy is furnished each day, unless the patient's medical needs indicate that daily therapy is required. For example, if physical therapy is furnished on 3 days each week and occupational therapy is furnished on 2 other days each week, the “daily basis” requirement would be satisfied only if there is a valid medical reason why both cannot be furnished on the same day. The basic issue here is not whether the services are needed, but when they are needed. Unless there is a legitimate medical need for scheduling a therapy session each day, the “daily basis” requirement for SNF coverage would not be met. • Medicare Benefit Policy Manual Chapter 8 – 20.1 • .
Medicare “No Improvement” Standard 30.4 - Direct Skilled Therapy Services to Patients (Rev. 179, Issued: 01-14-14, Effective: 01-07-14, Implementation: 01-07-14) A3-3132.1.C, SNF-214.1.C The following sections contain examples and guidelines concerning direct skilled therapy services to patients, including skilled physical therapy, occupational therapy, and speech/language pathology therapy. Coverage for such skilled therapy services does not turn on the presence or absence of a beneficiary’s potential for improvement from therapy services, but rather on the beneficiary’s need for skilled care. Therapy services are considered skilled when they are so inherently complex that they can be safely and effectively performed only by, or under the supervision of, a qualified therapist. (See 42CFR §409.32) These skilled services may be necessary to improve the patient’s current condition, to maintain the patient’s current condition, or to prevent or slow further deterioration of the patient’s condition. If all other requirements for coverage under the SNF benefit are met, such skilled therapy services are covered when an individualized assessment of the patient’s clinical condition demonstrates that the specialized judgment, knowledge, and skills of a qualified therapist are necessary for the performance of the rehabilitation services. Medicare Benefit Policy Manual Chapter 8 – 20.1
Examples of Swing Bed Care • The Medicare Benefit Policy Manual Chapter 8 has MANY examples of the types of patients that qualify for Swing Bed (SNF) care. And, great examples of skilled care • Physical Therapy – Occupational Therapy – Speech • Wound Care • IV Antibiotics • Medication Management • Teaching and training activities • • Teaching self-administration of injectable medications or a complex range of medications; • • Teaching a newly diagnosed diabetic to administer insulin injections, to prepare and follow a diabetic diet, and to observe foot-care precautions; • • Teaching self-administration of medical gases to a patient; • • Gait training and teaching of prosthesis care for a patient who has had a recent leg amputation; • • Teaching patients how to care for a recent colostomy or ileostomy; • • Teaching patients how to perform self-catheterization and self-administration of gastrostomy feedings; • • Teaching patients how to care for and maintain central venous lines, such as Hickman catheters; • • Teaching patients the use and care of braces, splints and orthotics, and any associated skin care; and • • Teaching patients the proper care of any specialized dressings or skin treatments.
REGULATORYRESOURCES • State Operations Manual – Appendix A (Rev. 183, 10-12-18) • State Operations Manual - Appendix W (Rev. 183,10-12-18) • StateOperationsManual -AppendixPP (Rev. 173,11-22-17) • Medicare Claims Processing Manuals – Updated in 2019 • Medicare Claims Processing Manual, Chapter 4 (Rev. 4295, 5-03-19) • Medicare Claims Processing Manual, Chapter 6 (Rev. 4247, 03-01-19) • Medicare Benefit Policy Manual Chapter 8 (Rev. 4202, 01-18-19)
Interpretative Guidelines -- Appendix PP New requirements for LTC facilities State Operations Manual AppendixPP Nov 22,2017 Swing Bed Revisions State OperationsManual AppendixA October 12,2018 Swing Bed Revisions State OperationsManual AppendixW October 12,2018
REGULATORYCHANGES October 2018 Resident Choice of Physician -Clarification Timelines for Reporting Abuse - New PASARR –Clarification Plan of Care – Additional language andClarification Provide Culturally-Competent and Trauma Informed Care –New Reconciliation of Pre-Discharge Medications with Post-Discharge Medications –New Dental Care – Clarification ofTimelines Transfer & Discharge – Information at Discharge Notification of Ombudsman Notification -New
Pre-Admission Tips If patient is being transferred from another facility – review the chart. Don’t just rely on “verbal report” Patient / Family Buy is very important. Will they agree to actively participating in the Swing Bed program? • Review record for medical necessity • Ask for input from other team members • Physician – Provider • Nursing • Rehab • Pharmacy • Social Work • Ensure you have the services that the patient will need (i.e. Speech??) • Determine attending physician and that they will accept patient • Obtain Pre-authorization for services (if not Medicare Part A) • Discuss Swing Bed stay with patient and/or family to ensure they are willing to participate in a Swing Bed program
Admission - Physician Tips If you use the same medical record – their still needs to be orders for Swing Bed • Discharge order from acute (if in same facility) • Order to admit to SwingBed • Orders for Swing Bedstay • New or updatedH&P • Initial certification or documentation of NEED for Swing Bed stay, expected length of stay and that care can only be reasonably provided on an inpatient basis
Patient Name: Admission Date: Health Insurance: Reason for Admission: Goals for Admission: Expected Length of Stay: Admission to swing bed is for the same condition(s) for which the (if no, please explain) c YES c NO Patient received inpatient hospital services CERTIFICATION I certify that services are required to be given on a daily basis which, Required at time as a practical matter, can be only be provided in a swing bed or skilled nursing facility. of admission Physician Signature Date and Time Certification – Specific Form Not Required
Admission Tips Some information must be provided verbally If patient cannot sign, review with decision maker and obtain signatures Designate responsibility for after-hours / weekends • Provide admission information to patient including resident rights, etc. • Review with patient (verbally) • Ensure signatures / documentation are in the medical record • Notify team members of admission • Schedule first multi-disciplinary meeting
PatientRequired Notices • Description of SwingBed • Resident Rights andResponsibilities • A description of Hospital’s policies regarding advancedirectives • A list of attending physicians who treatpatients • Resident Choice ofphysicians • Information on how to contact providers(ALL) • FinancialObligations • Transfer and Dischargepolicies • Notice of privacypractices • How to file grievance orcomplaint • Hospital responsibility for preventing patientabuse • Information for reporting Abuse andNeglect • Contact information for Hospital and State Agencies including State Ombudsman Information provided both orally and in writing in a language that the resident understands of his or her rights and all rules and regulations governing resident conduct and responsibilities during the stay in the facility. The facility must also provide the resident with the notice (if any) of the State developed under section 1919(e)(6) of theAct. Such notification must be made prior to or upon admission and during the resident’s stay. Receipt of such information, and any amendments to it, must be acknowledged inwriting A facility must promote the exercise of rights for all residents, including those who face barriers such as communication problems, hearing problems and cognitionlimits.
You have the right to a dignified existence, self-determination, and communication with and access to persons and services inside and outside the facility. • You have the right to be free of interference, coercion, discrimination, and reprisal from the facility in exercising your rights. You have the right to be supported by the facility in the exercise of your rights. • You have the right to be informed of, and participate in, your treatment, including the right to be fully informed in a language that you can understand of your total health status, including but not limited to, your medical condition. • You have the right to be informed, in advance, of changes to your plan of care. • You have the right to request, refuse, and/or discontinue treatment. • You have the right to participate in or refuse to participate in experimental research • You have the right to formulate an advance directive. • You have the right to choose an attending physician. You have the right to be informed if the physician you have chosen is unable or unwilling to be your attending physician, and to have alternative physicians discussed with you, and to honor your preferences, if any, in identifying options. • You have the right to be informed of the name, specialty, and way of contacting your physician and other primary care professionals responsible for your care. • You have the right to retain and use personal possessions, including furnishings, and clothing, as space permits, unless to do so would infringe upon the rights of health and safety or other residents. • You have the right to share a room with your spouse when your spouse is in the same facility, and both you and your spouse consent to the arrangement. • You have the right to immediate access by immediate family and other relatives, subject to your right to deny or withdraw consent at any time. • You have the right to immediate access by others who are visiting with your consent, subject to reasonable clinical and safety restrictions and your right to deny or withdraw consent at any time. • You have the right to choose to or refuse to perform services for the facility, and the facility must not require you to perform services for the facility. You may choose to perform services for the facility, when: • The facility has documented your need or desire to work in the plan of care; • Your plan of care specifies the nature of the services performed and whether the services are voluntary or paid; • You receive compensation for paid services at or above prevailing rates; and • You agree to the work arrangement described in the plan of care. Resident (Patient) Rights • You have the right to a dignified existence, self-determination, and communication with and access to persons and services inside and outside the facility. • You have the right to be free of interference, coercion, discrimination, and reprisal from the facility in exercising your rights. You have the right to be supported by the facility in the exercise of your rights. • You have the right to be informed of, and participate in, your treatment, including the right to be fully informed in a language that you can understand of your total health status, including but not limited to, your medical condition. • You have the right to be informed, in advance, of changes to your plan of care. • You have the right to request, refuse, and/or discontinue treatment. • You have the right to participate in or refuse to participate in experimental research • You have the right to formulate an advance directive. • You have the right to choose an attending physician. You have the right to be informed if the physician you have chosen is unable or unwilling to be your attending physician, and to have alternative physicians discussed with you, and to honor your preferences, if any, in identifying options. • You have the right to be informed of the name, specialty, and way of contacting your physician and other primary care professionals responsible for your care. • You have the right to retain and use personal possessions, including furnishings, and clothing, as space permits, unless to do so would infringe upon the rights of health and safety or other residents
You have the right to a dignified existence, self-determination, and communication with and access to persons and services inside and outside the facility. • You have the right to be free of interference, coercion, discrimination, and reprisal from the facility in exercising your rights. You have the right to be supported by the facility in the exercise of your rights. • You have the right to be informed of, and participate in, your treatment, including the right to be fully informed in a language that you can understand of your total health status, including but not limited to, your medical condition. • You have the right to be informed, in advance, of changes to your plan of care. • You have the right to request, refuse, and/or discontinue treatment. • You have the right to participate in or refuse to participate in experimental research • You have the right to formulate an advance directive. • You have the right to choose an attending physician. You have the right to be informed if the physician you have chosen is unable or unwilling to be your attending physician, and to have alternative physicians discussed with you, and to honor your preferences, if any, in identifying options. • You have the right to be informed of the name, specialty, and way of contacting your physician and other primary care professionals responsible for your care. • You have the right to retain and use personal possessions, including furnishings, and clothing, as space permits, unless to do so would infringe upon the rights of health and safety or other residents. • You have the right to share a room with your spouse when your spouse is in the same facility, and both you and your spouse consent to the arrangement. • You have the right to immediate access by immediate family and other relatives, subject to your right to deny or withdraw consent at any time. • You have the right to immediate access by others who are visiting with your consent, subject to reasonable clinical and safety restrictions and your right to deny or withdraw consent at any time. • You have the right to choose to or refuse to perform services for the facility, and the facility must not require you to perform services for the facility. You may choose to perform services for the facility, when: • The facility has documented your need or desire to work in the plan of care; • Your plan of care specifies the nature of the services performed and whether the services are voluntary or paid; • You receive compensation for paid services at or above prevailing rates; and • You agree to the work arrangement described in the plan of care. Resident (Patient) Rights • You have the right to share a room with your spouse when your spouse is in the same facility, and both you and your spouse consent to the arrangement. • You have the right to immediate access by immediate family and other relatives, subject to your right to deny or withdraw consent at any time • You have the right to immediate access by others who are visiting with your consent, subject to reasonable clinical and safety restrictions and your right to deny or withdraw consent at any time. • You have the right to choose to or refuse to perform services for the facility, and the facility must not require you to perform services for the facility. You may choose to perform services for the facility, when: • The facility has documented your need or desire to work in the plan of care; • Your plan of care specifies the nature of the services performed and whether the services are voluntary or paid • You receive compensation for paid services at or above prevailing rates; and • You agree to the work arrangement described in the plan of care. • 15. You have the right to be informed in writing, if you have Medicaid insurance, at the time of admission or when you become eligible for Medicaid of: • The items and services that are included in nursing facility services under the State plan and for which you may not be charged • Those other items and services that the Hospital offers and for which you may be charged, and the amount of charges for those services • Be informed when changes are made to items and services • 16. You have the right to be informed before, or at the time of admission, and periodically during your stay, of services available in the facility and of charges for those services, including any charges for services not covered under Medicare/Medicaid or by the facility’s per-diem rate. • You have the right to privacy in your accommodations. • You have the right to privacy for any medical treatment or personal care. • 19. You have the right to privacy for visits and meetings with family and resident groups. This does not require the facility to provide you with a private room.
You have the right to a dignified existence, self-determination, and communication with and access to persons and services inside and outside the facility. • You have the right to be free of interference, coercion, discrimination, and reprisal from the facility in exercising your rights. You have the right to be supported by the facility in the exercise of your rights. • You have the right to be informed of, and participate in, your treatment, including the right to be fully informed in a language that you can understand of your total health status, including but not limited to, your medical condition. • You have the right to be informed, in advance, of changes to your plan of care. • You have the right to request, refuse, and/or discontinue treatment. • You have the right to participate in or refuse to participate in experimental research • You have the right to formulate an advance directive. • You have the right to choose an attending physician. You have the right to be informed if the physician you have chosen is unable or unwilling to be your attending physician, and to have alternative physicians discussed with you, and to honor your preferences, if any, in identifying options. • You have the right to be informed of the name, specialty, and way of contacting your physician and other primary care professionals responsible for your care. • You have the right to retain and use personal possessions, including furnishings, and clothing, as space permits, unless to do so would infringe upon the rights of health and safety or other residents. • You have the right to share a room with your spouse when your spouse is in the same facility, and both you and your spouse consent to the arrangement. • You have the right to immediate access by immediate family and other relatives, subject to your right to deny or withdraw consent at any time. • You have the right to immediate access by others who are visiting with your consent, subject to reasonable clinical and safety restrictions and your right to deny or withdraw consent at any time. • You have the right to choose to or refuse to perform services for the facility, and the facility must not require you to perform services for the facility. You may choose to perform services for the facility, when: • The facility has documented your need or desire to work in the plan of care; • Your plan of care specifies the nature of the services performed and whether the services are voluntary or paid; • You receive compensation for paid services at or above prevailing rates; and • You agree to the work arrangement described in the plan of care. Resident (Patient) Rights • You have the right to privacy in your oral (spoken), written, and electronic communications, including the right to send and promptly receive unopened mail and other letters, packages and other materials delivered to the facility for you, including those delivered through a means other than a postal service. • You have the right to access to stationery, postage, and writing implements at your own expense. • You have the right to secure and confidential personal and medical records. You have the right to refuse the release of personal and medical records except as required or provided by federal or state laws. The facility must allow representatives of the Office of the State Long-Term Care Ombudsman to examine your medical, social, and administrative records in accordance with State law. • You have the right to remain in the facility, and not be transferred or discharged unless: • The transfer or discharge is necessary for your welfare, and your needs cannot be met in the facility • The transfer or discharge is appropriate because your health has improved sufficiently so that you no longer need the services provided by the facility • The safety of individuals in the facility are endangered due to your clinical or behavioral status • The health of individuals in the facility would be endangered • You have failed, after reasonable and appropriate notice, to pay for (or to have paid under Medicare or Medicaid) a stay at the facility. Non-payment applies if you do not submit the necessary paperwork for third-party payment or after the third party, including Medicare or Medicaid, denies the claims and you refuse to pay for your stay. • The facility ceases to operate • The facility may not transfer or discharge you while an appeal is pending, unless the failure to discharge or transfer would endanger the health or safety of you or other individuals in the facility. • 24. You have the right to be free from abuse, neglect, misappropriation of property, and exploitation. This includes but is not limited to freedom from corporal punishment, involuntary seclusion, and any physical or chemical restraint not required to treat your medical symptoms.
You have the right to a dignified existence, self-determination, and communication with and access to persons and services inside and outside the facility. • You have the right to be free of interference, coercion, discrimination, and reprisal from the facility in exercising your rights. You have the right to be supported by the facility in the exercise of your rights. • You have the right to be informed of, and participate in, your treatment, including the right to be fully informed in a language that you can understand of your total health status, including but not limited to, your medical condition. • You have the right to be informed, in advance, of changes to your plan of care. • You have the right to request, refuse, and/or discontinue treatment. • You have the right to participate in or refuse to participate in experimental research • You have the right to formulate an advance directive. • You have the right to choose an attending physician. You have the right to be informed if the physician you have chosen is unable or unwilling to be your attending physician, and to have alternative physicians discussed with you, and to honor your preferences, if any, in identifying options. • You have the right to be informed of the name, specialty, and way of contacting your physician and other primary care professionals responsible for your care. • You have the right to retain and use personal possessions, including furnishings, and clothing, as space permits, unless to do so would infringe upon the rights of health and safety or other residents. • You have the right to share a room with your spouse when your spouse is in the same facility, and both you and your spouse consent to the arrangement. • You have the right to immediate access by immediate family and other relatives, subject to your right to deny or withdraw consent at any time. • You have the right to immediate access by others who are visiting with your consent, subject to reasonable clinical and safety restrictions and your right to deny or withdraw consent at any time. • You have the right to choose to or refuse to perform services for the facility, and the facility must not require you to perform services for the facility. You may choose to perform services for the facility, when: • The facility has documented your need or desire to work in the plan of care; • Your plan of care specifies the nature of the services performed and whether the services are voluntary or paid; • You receive compensation for paid services at or above prevailing rates; and • You agree to the work arrangement described in the plan of care. Resident (Patient) Rights in a language that the resident understandsorally and in writing
FINANCIALOBLIGATIONS 1 • Inform each resident who is entitled to Medicaid benefits, in writing, at the time of admission to the nursing facility or, when the resident becomes eligible for Medicaidof-- • The items and services that are included innursingfacilityservices under the State plan and for which the resident may not be charged; • Those other items and services that the facility offers andforwhichthe resident may be charged, and the amount of charges for those services; and • Inform each resident when changes are made to the items and services specified in paragraphs (5)(i)(A) and (B) of thissection. • (6) The facility must inform each resident before, or at the time of admission, and periodically during the resident’s stay, of services available in the facility and of charges for those services, including any charges for services not covered under Medicare or by the facility’s per diem rate. • Medicare • $0 for the first 20 days of each benefitperiod • $170.50 per day for days 21–100 of each benefitperiod(2019) ASSIGN SOMEONE TO UPDATE EACHYEAR! • All costs for each day 101 andbeyond
Choice of Physicians & Info on Contacting Providers C-0361§483.10(d): Choice of attending physician. The resident has the right to choose his or her attending physician. The physician must be licensed to practice,and If the physician chosen by the resident refuses to or does not meet requirements specified in this part, the facility may seek alternate physician participation as specified in paragraphs (d)(4) and (5) of this section to assure provision of appropriate and adequate care andtreatment. The facility must ensure that each resident remains informed of the name, specialty, and way of contacting the physician and other primary care professionals responsible for his or hercare. The facility must inform the resident if the facility determines that the physician chosen by the resident is unable or unwilling to meet requirements specified in this part and the facility seeks alternate physician participation to assure provision of appropriate and adequate care and treatment. The facility must discuss the alternative physician participation with the resident and honor the resident's preferences, if any, amongoptions. If the resident subsequently selects another attending physician who meets the requirements specified in this part, the facility must honor thatchoice.
After Admission Tips Assign responsibility for each assessment component. Timelines need to be congruent with your length of stay Don’t forget assessment of trauma Don’t forget review of PASRR (if patient has one completed in another facility) • Complete comprehensive assessment (each discipline) per facility timelines • Include assessment of trauma • Develop multi-disciplinary care plan of care • attendingphysician • registered nurse with responsibility for theresident • nurse aide with responsibility for theresident • member of food and nutrition servicesstaff • patient
COMPREHENSIVEASSESSMENT C-0388§485.645(d)(6): Comprehensive assessment, comprehensive care plan, and discharge planning (§483.20(b),and §483.21(b) and (c)(2) of this chapter), except that the CAH is not required to use the resident assessment instrument (RAI) specified by the State that is required under §483.20(b), or to comply with the requirements for frequency, scope, and number of assessments prescribed in §413.343(b) of thischapter. §483.20(b): Comprehensiveassessments— (1) Resident assessment instrument. A facility must make a comprehensive assessment of a resident's needs, strengths, goals, life history and preferences, using the resident assessment instrument (RAI) specified by CMS. Theassessment must include at least thefollowing: CAHs are exempt from completing aMDS C-0388§485.645(d)(6): The CAH is not required to use the resident assessment instrument (RAI) specified by the State thatis required under §483.20(b), or to comply with the requirements for frequency, scope, and number of assessments prescribedin §413.343(b) of this chapter). Also, note that CAHs are not required to complete thePASARR. However, if a patient had a PASARR completed by a facility that was required to do so prior to admission into a CAH swing bed, the recommendations from the PASARR should be included in the CAHs comprehensive treatment plan for thepatient.
CAH - COMPREHENSIVEASSESSMENT The facility must conduct initially and periodically a comprehensive, accurate, standardized, reproducible assessmentof each resident’s functionalcapacity The assessment must include at leastthe following: Identification and demographicinformation Customaryroutine Cognitivepatterns Communication Vision Mood and behaviorpatterns Psychosocial well-being – HISTORYof traumatic events (October2018) Physical functioning and structuralproblems Continence Disease diagnoses and healthconditions Dental and nutritionalstatus Skincondition Activitypursuit Medications Special treatments andprocedures Dischargepotential REVIEW PASSAR – if one has beendone
Rural Hospitals PPS - ASSESSMENT Hospitals with swing beds paid under PPS must utilize and submit the Swing Bed MDS to CMS There are 9 different item subsets for nursing homes and 5 for swing bed providers: Source: Long-Term Care Facility Resident Assessment Instrument 3.0 User’s Manual Version 1.17, October 2019
Nutrition • Nutrition andHydration • NutritionAssessment • NutritionRecommendations • Documentation of hydration status (IMPORTANT!) • C-0410 §483.25(g): Assisted nutrition and hydration. (Includes naso-gastric and gastrostomy tubes, both percutaneous endoscopic gastrostomy and percutaneous endoscopic jejunostomy, and enteral fluids). Based on a resident's comprehensive assessment, the facility must ensure that a resident— (1) Maintains acceptable parameters of nutritional status, such as usual body weight or desirable body weight range and electrolyte balance, unless the resident's clinical condition demonstrates that this is not possible or resident preferences indicate otherwise; • (2) Is offered sufficient fluid intake to maintain proper hydration and health Interpretive Guidelines §485.645(d)(9)
Activities • Activities Assessment • Activities Plan • Documentation of Activities status (IMPORTANT!) • C-0385 (Rev. 183, Issued: 10-12-18, Effective: 10-12-18, Implementation: 10-12-18) • §483.24(c) Activities. • (1) The facility must provide, based on the comprehensive assessment and care plan and the preferences of each resident, an ongoing program to support residents in their choice of activities, both facility-sponsored group and individual activities and independent activities, designed to meet the interests of and support the physical, mental, and psychosocial well-being of each resident, encouraging both independence and interaction in the community.
Activities C-0385(Rev. 183, Issued: 10-12-18, Effective: 10-12-18, Implementation: 10-12-18) §485.645(d)(4) Patient Activities (§483.24(c) of this chapter), except that the services may be directed either by a qualified professional meeting the requirements of §483.24(c)(2), or by an individual on the facility staff who is designated as the activities director and who serves in consultation with a therapeutic recreation specialist, occupational therapist, or other professional with experience or education in recreational therapy. (2) The activities program must be directed by a qualified professional who is a qualified therapeutic recreation specialist or an activities professional who— (i) Is licensed or registered, if applicable, by the State in which practicing; and (ii) Is: (A) Eligible for certification as a therapeutic recreation specialist or as an activities professional by a recognized accrediting body on or after October 1, 1990; or (B) Has 2 years of experience in a social or recreational program within the last 5 years, one of which was full-time in a therapeutic activities program; or (C) Is a qualified occupational therapist or occupational therapy assistant; or (D) Has completed a training course approved by the State.
CAH - Comprehensive ASSESSMENT TIMELINE • The new CoPs eliminate the requirement for specific timelines for Swing Beds in a CAH (7 day and 14 day timelines are notapplicable). • However, timelines must be congruent with your LengthofStay. Forexample: • Nursing within 24hours • Rehab within 48hours • Dietary within 48hours • Activities within 48hours • Social Services / Discharge Planning within 48hours • Pharmacy, if appropriate, within 48hours
REASSESSMENT AFTER SIGNIFICANTCHANGE • A “significant change” may include, but is not limited to, any of the following, or may be determined by a MD/DO’s decision if uncertaintyexists. • Deterioration in two of more activities of daily living (ADLs), or any combination of deterioration in two ormore areas of ADLs, communication, or cognitive abilities that appear permanent. For example, pronounced deterioration in function and communication following astroke. • Loss of ability to ambulate freely or to use hands to grasp small objects to feed or groom oneself, suchas spoon, toothbrush, or comb. Temporary loss of ability, such as during an acute illness, is notincluded. • Deterioration in behavior or mood, to the point where daily problems arise or relationships have become problematic and staff conclude that these changes in the resident’s psychosocial status are not likely to improve without staffintervention. • Deterioration in a resident’s health status, where this change places the resident’s life in danger (e.g., stroke, heart disease, metastatic cancer); where the change is associated with a serious clinical complication (e.g., initial development of a stage III pressure sore, prolonged delirious state, or recurrent decline in level of consciousness); or change that is associated with an initial diagnosis of a condition that is likely to affect the resident’s physical, mental, or psychosocial well-being over a prolonged period of time (e.g., Alzheimer’s disease or diabetes); or the onset of significant, unplanned weight loss (5% in the last 30 days, 10% in the last 180days).
TRAUMA INFORMEDCARE Trauma Informed Care is an organizational structure and treatment framework that involves understanding, recognizing, and responding to the effects of all types of trauma. Trauma Informed Care also emphasizes physical, psychological and emotional safety for both consumers and providers, and helps survivors rebuild a sense of control andempowerment. http://traumainformedcareproject.org/index.php
TRAUMA INFORMEDCARE 1. Has there been anything within the last six months to a year that has caused you to be upset or very worried? 2. Have you experienced the loss of a close friend, relative or a pet that you loved recently? 3. Have you had any past trauma in your life that we should know about so we can better care for you? 4. If you have experienced some kind of trauma is there something that helps you feel better? 5. Is there anything we can do to help while you are in the (Hospital/Nursing Home) DON’T PROBE – NO IS NO
Important Note The assessment is not JUST A NURSING ASSESSMENT – It’s Multi-disciplinary Important Note This is not AN ACUTE CARE ASSESSMENT Important Note Assessment must include direct OBSERVATION and COMMUNICATION with the patient Important Note Assessment must include communication / input with licensed and non-licensed DIRECT CARE STAFF MEMBERS ON ALL SHIFTS
COMPREHENSIVE CAREPLAN Timelines must be congruent with your Length ofStay. Forexample: IDT meeting within 48 – 72 hours of admission to develop comprehensive plan ofcare. C-0388§485.645(d)(6) (ii) Prepared by an interdisciplinary team, that includes but is not limitedto— The attendingphysician. A registered nurse with responsibility for theresident. A nurse aide with responsibility for theresident. A member of food and nutrition servicesstaff. To the extent practicable, the participation of the resident and the resident's representative(s). An explanation must be included in a resident's medical record if the participation of the resident and their resident representative is determinednot practicable for the development of the resident's careplan. Other appropriate staff or professionals in disciplines as determined by the resident's needs or as requested by theresident. (iii) Reviewed and revised by the interdisciplinary team after each assessment, including both the comprehensive andquarterly reviewassessments. (3) The services provided or arranged by the facility, as outlined by the comprehensive care plan,must— Meet professional standards ofquality. Be provided by qualified persons in accordance with each resident's written plan ofcare. Be culturally-competent andtrauma-informed