Download
1 / 61
730 likes | 3.45k Vues
Learn about the history, anatomy, histology, and classification of parotid tumors. Includes detailed information on the incidence, etiology, and presentation of these tumors, with a focus on surgical implications and treatment options.

E N D
PAROTID TUMORS Dr. Ashith Shetty Moderator-Dr. Anand I. P
History Thomas Wharton, a London physician, described the submandibular duct. Neils Stensen discovered the parotid duct in1660. John Hunter resected a parotid tumor in 1785. Thomas Cawardine, a member of the surgical staff of the Bristol Royal Infirmary first suggested the facial nerve be identified.
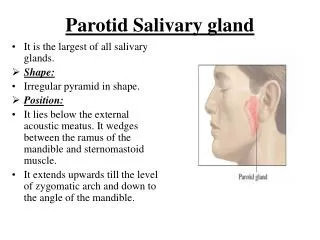
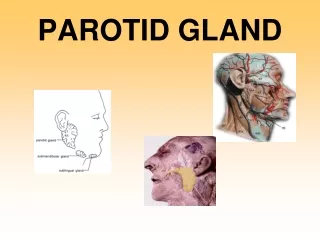
Anatomy Parotid gland is the largest serous salivary gland and is also called the queen of the face Parotid; para-around ; otic-ear They produce saliva which keeps the oral cavity moist, helps in chewing and swallowing and also contain enzymes that aid digestion.
Largest of the three salivary glands, weighing from 14-28g. Situated below the external acoustic meatus, between the ramus of mandible and mastoid process with the sternocleidomastoid muscle. The investing layer of the deep cervical fascia splits to form a capsule; parotid capsule, and is attached above to the zygomatic arch.
The gland is divided into 2 parts: • Superficial part(80%)- overlies the masseter and mandible • Deep part(20%)-lies behind the mandible and medial pterygoid muscle
The parotid duct (Stensen’s duct), 5cm in length, emerges from the middle of the anterior border of the gland, runs over masseter muscle, passes through buccinator muscle and opens into the oral mucosa opposite to the crown of upper 2nd molar An accessory part of the parotid gland if present is usually found adjacent to the parotid duct in the buccal space
Structures within the parotid gland (from deep to superficial): • External carotid artery, maxillary artery, superficial temporal artery, posterior auricular artery, transverse facial artery • Retromandibular vein formed by fusion of maxillary and superficial temporal veins • Facial nerve with its branches
Facial nerve: • Emerges from stylomastoid foramen lying between external auditory meatus and mastoid process • Passes around the neck of the condyle of mandible and becomes superficial, later dividing into temporofacial and cervicofacial branches which in turn divides into many branches • Some of these may be interconnected as pes anserinus • Branches are- temporal, zygomatic, buccal, mandibular and cervical
Facio-venous plane of Patey is of surgical importance. The facial nerve along with the retromandibular vein is present in this plane.
Blood supply: • Arterial- external carotid artery and its branches • Venous- external jugular vein • Nerve supply: • Parasympathetic nerves- is secretomotor from auriculotemporal • Sympathetic is vasomotor from plexus around the external carotid artery • Sensory nerve comes from the auriculotemporal nerve • Lymphatic drainage: parotid nodes
Histology In major salivary glands, both serous and mucous cells are arranged into acini, which are drained by series of ducts- an intercalated duct that drains into a striated duct, which empties into an excretory duct Contractile myoepithelial cells surround acini and intercalated ducts- help in draining saliva Serous acini predominate in parotid gland Mucinous acini abundant in sublingual and minor salivary glands Serous and mucous acini in submandibular gland
INCIDENCE Majority of the salivary gland tumors arise from the parotid gland Highest incidence seen in the Eskimos of Greenland
Etiology • Radiation • Ionizing radiation • Ultraviolet radiation • Age of onset- 12- 16 years after exposure • Viruses • Role of Ebstein-Barr virus • Genetic factors
Others • Occupational exposure- asbestos and rubber industries • Hormonal effect- women with history of early menarche and nulliparity • Warthin’s tumor strongly associated with cigarette smoking
Classification • EPITHELIAL (90%) • BENIGN • PLEOMORPHIC ADENOMAS • WARTHIN’S TUMOR • OXYPHIL ADENOMA • MALIGNANT • MUCOEPIDERMOID CARCINOMA • ADENOCARCINOMA • ADENOID CYSTIC CARCINOMA • EPIDERMOID CARCINOMA • UNDIFFERENTIATED CARCINOMA • CARCINOMA ARISING FROM PLEOMORPHIC ADENOMA
NON-EPITHELIAL TUMORS • HEMANGIOMA • FIBROMA • LIPOMA • LYPHANGIOMA • LYMPHOMA • SARCOMA C. METASTATIC TUMORS
WHO CLASSIFICATION • ADENOMAS • PLEOMORPHIC ADENOMA • MYOEPITHELIOMA (MYOEPITHELIAL ADENOMA) • BASAL CELL ADENOMA • WARTHIN’S TUMOR • ONCOCYTOMA (OXYPHIL ADENOMA) • CARCINOMAS • ACINIC CELL CARCINOMA • MUCOEPIDERMOID CARCINOMA • ADENOID CYSTIC CARCINOMA
ADENOCARCINOMA • CARCINOMA IN PLEOMORPHIC ADENOMA • SQUAMOUS CELL CARCINOMA (EPIDERMOID CA) • UNDIFFERENTIATED CARCINOMA • NONEPITHELIAL TUMORS • MALIGNANT LYMPHOMAS • SECONDARY TUMORS • UNCLASSIFIED TUMORS • TUMOR LIKE LESIONS
PRESENTATION Complex and diverse group of tumors Diversity of histopathologic patterns Different degree of aggressiveness and pattern of spread
Presentation Both benign and malignant tumors of parotid gland usually present as a painless swelling Growth of these tumors is so slow that patients often wait many months or years before seeking attention Raised ear lobule Cannot be moved above the zygomatic arch- curtain sign Deviation of uvula and tonsil towards midline in case of deep lobe involvement
Features indicative of malignancy • facial nerve paresis or paralysis • Pain • Fixation of mass to overlying skin or underlying structures • Associated cervical adenopathy
Pleomorphic adenoma The most common benign salivary gland tumor Also known as mixed tumor More common in females,3rd to 4th decade 80% are within the superficial lobe
Derived from mixture of epithelial and myoepithelial cells They reveal epithelial elements dispersed throughout a matrix along with a varying degree of myxoid, hyaline, cartilaginous and even osseous tissue They produce mucoid material Morphology- they are well demarcated masses. Although encapsulated, in some locations the capsule is not fully developed. The cut surface is grey white with myxoid and blue translucent areas of chondroid
Clinical features: • Painless slow growing mass • Usually unilateral • Smooth, firm, lobulated, mobile swelling • Present as a swelling in front, below and behind ear • Raises the ear lobule • Curtain sign +ve • Obliteration of the retromandibular groove
Sometimes when deep lobe is involved, presents as a swelling in lateral wall of pharynx, soft palate and posterior pillar of the fauces. There may not be any visible swelling in the preauricular region, called as dumb bell tumor. • Long standing pleomorphic adenoma may turn into carcinoma (ca. in ex. Pleomorphic adenoma) • Recurrent pleomorphic adenoma- seen following incomplete tumor removal or spillage of the tumor during surgery.
Investigations: • FNAC • CT scan • MRI • Technetium scan- cold spot (incision biopsy of parotid tumor is contraindicated as chances of seedling, injury to facial nerve and recurrence are high)
Treatment: • Surgery- if only superficial lobe involved; superficial parotidectomy • If both lobes involved- total conservative parotidectomy preserving facial nerve • Treatment of malignant pleomorphic adenoma: • Radical parotidectomy, if facial nerve involved • Advanced tumors with fixed nodes may require post op radiotherapy
Warthin’s tumor Also known as adenolymphoma or papillary cystadenoma lymphomatosum Most common monomorphic adenoma 2nd most common tumor-10% of parotid tumors Develops only in the parotid gland Peak incidence- 60-70 years Predominantly in men
Histology: • Consists of a characteristic eosinophilic, glandular epithelial component and a stroma of lymphocytes which may form follicles or cysts • Morphology: • Most are round to oval, encapsulated masses, mostly arising in the superficial parotid gland • Transection reveals a pale grey surface punctated by narrow cystic or cleft like spaces filled with a mucinous or serous secretion • these spaces are lined by double layer of neoplastic epithelial cells resting on dense lymphoid stroma • Double layer of lining cells is distinctive having an abundant, finely granular, eosinophilic cytoplasm, imparting an oncocytic appearance
Clinical features: • Slow growing, smooth, round border with soft, cystic consistency situated in the lower pole • Multifocal and bilateral • Smokers have higher risk • Investigations: • FNAC • Technetium scan-hot spot • Treatment: • Enucleation to be done, since it is got a well defined capsule
Oncocytoma Rare tumors , also known as Oxyphilic adenoma Predominantly in women in the 7th or 8th decade Parotid gland- most frequent site Benign tumor containing oncocytes (eosinophilic cells) with granular cytoplasm6 Slow growing, smooth rubbery mass and rarely bilateral Treatment- excision is curative
Mucoepidermoid carcinoma Commonest malignant salivary gland tumor Contains two major elements-mucin producing cells and epithelial cells of epidermoid variety MEC consists approximately 35% salivary gland malignancy
Mucoepidermoid CarcinomaLOW GRADE / HIGH GRADE
Types: • Low grade- well differentiated, predominance of mucus secreting cells and well differentiated epidermoid cells • Intermediate grade- moderately differentiated • High grade- poorly differentiated, shows few or no mucus producing cells and poorly differentiated epidermoid cells • The grading system of MEC also correlates with the prognosis • Patients with high grade tend to present with more advanced stage disease and high incidence of nodal involvement, recurrence, metastasis and worse survival rate
Morphology: • Apparently circumscribed, lack well defined capsules and often infiltrative at margins • Pale and grey white on transection reveal small mucin containing cysts • Histologic pattern is that of cords, sheets or cystic configuration of squamous, mucus or intermediate cells
Clinical features • Swelling in parotid or submandibular region • Slowly progressive, eventually attaining a large size • Hard, nodular often with involvement of skin and lymph nodes • Facial nerve involvement is late • Treatment: • Low grade- complete excision of tumor • High grade-needs post op radiation • In neck metastasis- neck dissection
Adenoidcystic carcinoma • Most common malignant tumor in submandibular gland • Peak incidence in 5th and 6th decade of life • Slightly more common among females • Very aggressive tumor • Described in 3 histological sub types: • Cribriform • Tubular • Solid (worst prognosis)
Peculiar tendency to spread along nerves • Perineural infiltrates for a long distance in the perineural tissue of adjacent nerves and may invade medullary bone inducing significant bone resorption • Morphology: • Grossly- small, poorly encapsulated, infiltrative grey pink lesions • Histologically composed of small cells having dark compact nuclei and scant cytoplasm