Engineering Antibodies (2) Immunotherapeutic Examples MSc Programme University of Nottingham 14 th February 2005
Explore immunotherapeutic examples in engineering antibodies for tumor therapy, organ transplantation, and auto-immunity treatments. Learn about the role of different antibodies and their effectiveness in various medical applications. Discover the ideal properties of antibodies for specific therapies using cutting-edge research examples.

Engineering Antibodies (2) Immunotherapeutic Examples MSc Programme University of Nottingham 14 th February 2005
E N D
Presentation Transcript
Engineering Antibodies (2)Immunotherapeutic ExamplesMSc Programme University of Nottingham14th February 2005 by Mike Clark, PhD Department of Pathology Division of Immunology Cambridge University UK www.path.cam.ac.uk/~mrc7/
University Research Programmes • Immunosuppression • CD4, CD3, monovalent CD3, CD52 (Campath) • Tumour Therapy • CD52 (Campath), bispecific CD3 • Organ Transplantation • CD52, CD3, CD4, synergistic CD45 pair • Allo and auto-immunity • RhD, HPA-1a • Chronic Inflammation • CD18, VAP-1
Declaration of interests (rights as an inventor) • CD52 IlexOncology/Genzyme (Campath® humanisation) • CD4 TolerRx/Genentech (for induction of tolerance) • CD4 BTG (improved method of humanisation) • CD3 BTG /TolerRx (immunosuppression and tolerance) • CD18 Millennium Pharmaceuticals • VAP-1 BioTie / University collaboration • RhD NBS / University collaboration • HPA-1a NBS / University collaboration
Antibodies (eg CD52 Campath) can be effective in killing cancer cells (BCLL)
Fetomaternal alloimmune thrombocytopenia • Maternal IgG raised against fetal platelet alloantigens can cross the placenta and cause fetal platelet destruction • If the fetal platelet count falls dangerously low, cerebral hemorrage or death may result • Current therapies are intrauterine platelet transfusion and maternal therapy with high dose IVIG
Can a protective antibody be developed? • 90% severe cases FMAIT are due to antibodies against the alloantigen HPA-1a on GPIIIa • Single B cell epitope (Leu-33) could be blocked to prevent the binding of harmful antibodies • Outcome depends on antibody titre • Williamson et al. Blood 1998; 92: 2280 • Jaegtvik et al. Br J Obs Gynae 2000; 107: 691
Ideal properties of an antibody for FMAIT therapy • HPA-1a specificity (B2 variable regions) • able to cross the placenta • inactive in FcgR-mediated cell destruction • unable to activate complement
RhD HPA-1a
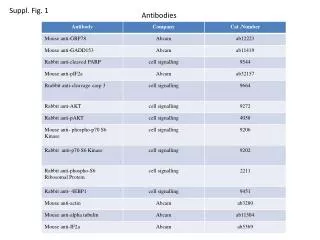
Chemiluminescent response of human monocytes to sensitised RBC Fog-1 140 antibodies 120 G1 G1D a 100 G1D b 80 G1D c % chemiluminescence 60 G1D ab 40 G1D ac G2 20 G2D a 0 G4 -20 G4D b 0 5000 10000 15000 20000 25000 30000 G4D c antibody molecules/cell
100 90 G1D b 80 G1D c 70 G1D ab 60 G1D ac 50 G2 % chemiluminescence 40 G2D a 30 G4D b G4D c 20 10 0 0.1 1 10 100 1000 inhibitorconcentration, m g/ml Inhibition of chemiluminescent response due to 2 mg/ml Fog-1 G1 by other Fog-1 antibodies
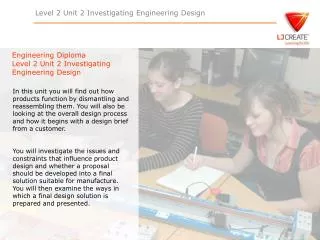
Inhibition by Fog-1 antibodies of ADCC due to clinically relevant polyclonal anti-RhD (at 3ng/ml) 120 100 80 G1D ab G2 G2D a 60 % RBC lysis G4 G4D b 40 20 0 0.1 1 10 100 1000 10000 inhibitor antibody concentration, ng/ml
HuVAP antibody VAP-1
Capture • and rolling 2. Activation 3. Stationary adhesion Free flow 4. Migration Integrin Chemokine signal Selectins IgSF Infection Multistep paradigm of neutrophil adhesion Endothelium
Amines Toxic aldehydes & H202 VAP-1 Role of VAP-1 sVAP-1 Modified Fc region Anti VAP-1 Selectin
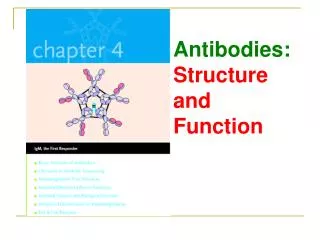
1. Capture and FcR ligation 2. Activation and integrin expression 3. Ultra-rapid stationary adhesion Fc receptor Anti VAP-1 IgG 2 Integrin IgSF like motif Microslide Flow Neutrophil adhesion assay VAP-1
Brief Acknowledgements Mike Clark Dept of Pathology Kathryn Armour Chris Kirton Cheryl Smith Lorna Williamson National Blood Service & Transfusion Medicine