Transplantation
Transplantation. Jeffrey J. Kaufhold, MD FACP Nephrology Associates December 2003. Transplantation Summary. Trends in Survival after transplant Donor and Recipient preparation HLA Matching Surgical Procedure Rejection diagnosis and treatment Immunosuppression

Transplantation
E N D
Presentation Transcript
Transplantation Jeffrey J. Kaufhold, MD FACP Nephrology Associates December 2003
TransplantationSummary • Trends in Survival after transplant • Donor and Recipient preparation • HLA Matching • Surgical Procedure • Rejection diagnosis and treatment • Immunosuppression • Infectious complications after Transplant • Other complications after Transplant • Kidney Pancreas Update • Immunology and Tolerance
Scope of problem • 300,000 dialysis patients in US • 55,000 patients on waiting List • 17,000 recovered kidneys per year • 11000 from “deceased donors” • 6000 from living related donors • 1000 kidneys not used after recovery • Average waiting time 5 years !
History of Transplants • 1950’s First attempted in Twins • Still rejected due to minor antigen differences • 1960’s First success • Imuran and Prednisone, ATG • 1983 Cyclosporine A introduced • Dramatic improvement in graft survival • Opened the era for success in Heart, lung, liver and other arenas.
Patient Survival 1 yr LRD 98% DD 95 Allograft Survival 1 yr LRD 95% DD 89 Allograft half-life LRD 21 years 5 yrs LRD 91 % DD 81 5 years LRD 76% DD 61 DD 13.8 years Survival after Transplant2003
Transplant survival • Relative risk of death • Transplanted in 1993 = 1.0 • Transplanted in 1998 = 0.74 • Currently on Wait list = 1.7 • These are the healthy ones! • Patients not on wait list = 2.6
Trends in Transplantation • Overall Mortality is unchanged! • Death with functioning graft increasing • Donor Age older • Recipient age is older • Time on waiting list is longer • Older, sicker patients are getting transplants
Transplant Update • Annual Death Rates • Pts on list 6.3 % • Diabetic pts on list 10.8 % • Pts not on list 21 % • Note that “death censored graft loss” is standard measure used in transplant outcome reports since this is desired outcome.
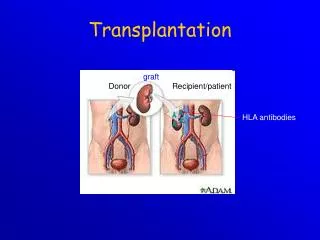
Donor Criteria • Living related preferred • Living unrelated next • Deceased Donor means longer wait • Brain death required • No Infection • No malignancy (except CNS lymphoma) • Preferrably under 60 years old • Normal renal function
Recipient Preparation • Dialysis or near Dialysis • GFR < 15 ml/min • Compliant with meds and treatment • Screen for infection, malignancy • Blood tests and colonoscopy • Screen for Heart Disease • Higher risk for dialysis pts • 25 y.o. on dialysis has same risk as 55 y.o. • Risk for dialysis pt 10 fold higher at any age.
Surgical Transplantation • Procedure time 2 - 4 hours • Hernia incision to expose Iliac A and V, extend to expose bladder • Retroperitoneal so recovery time from surgery is minimal • Anastomose Artery and Vein • Tunnel ureter into bladder • Lich, Ledbetter
Surgical Transplantation • The native kidneys are left intact • Unless problems with infection, HTN • Allograft is easy to palpate, biopsy • Ureter length is kept short • Where does the ureter get its blood supply?
Surgical Transplantation • The native kidneys are left intact • Unless problems with infection, HTN • Allograft is easy to palpate, biopsy • Ureter length is kept short • Dual Blood supply from renal artery and from cystic artery. Ischemic ureter leads to stricture or leak. • Warm ischemia time is kept to < 45 min • Cold ischemia time up to 72 hours!
Surgical Transplantation • Typical Scenario: • Multiple organ donor identified, blood typed • Organ recovery team takes abdominal organs first, heart and lungs last. (bone skin corneas may be taken after heart stops). • Organs are perfused and stored in preservative solution • Mixture of high K, antioxidants • Kept cold on ice. • Lymph Nodes, spleen used for HLA typing
Surgical Transplantation • Cold Storage limits for organs: • Heart 6 hours • Lung 6 hours • Pancreas 12 hours • Liver 24 hours • Kidney 72 hours + • Primary graft failure rate higher after 72 hrs. • Tissue weeks to months! • Bone, skin, cornea, dura mater, etc.
Surgical Transplantation • UNOS master list used to determine where organs sent, which pts are best match • Primary patient, plus a standby are called • Crossmatch takes 6 hours • Standby used if CM + or primary not available • A single Txp team could then do • SPK first (4-6 hours) • Liver next (8-12 hours) • Kidney last (2-4 hours)
Higher risk Deceased donor Recipient over 60 Donor over 60 Recipient race Black / Hispanic Long Cold Ischemic time Previous Txp High PRA Lower Risk Living donor Recipient under 60 Donor under 60 Recipient race Asian Short cold ischemia Higher HLA match Low PRA Risk of Graft Loss
Expanded Donor Kidneys • Used when risk of Txp is better than life expectancy on dialysis • Criteria • Recipient/donor over 60 • Diabetics over 40 • Failing access for dialysis • Patient with poor Quality of Life
Transplant Update • HLA Matching • Main HLA groups A B C D • C not important for transplant survival • Host of minor antigens • Most important antigens are B and D • A and B are constitutive (always expressed) • D antigen is inducible and responsible for more serious (vascular) rejections when it gets expressed.
Waiting list management • Point system for UNOS Wait list • 1 pt per year on list • 7 pts for 0 mismatch with B, DR antigens • 5 pts for 1 mm with B, DR • 2 pts for 2 mm with B, DR • 4 pts for match in pt with PRA > 80 % • 4 pts for Age < 11, 3 pts for age 11-18 • National sharing of 0 mismatch kidneys • 17-20 % of all transplants
Transplant Costs • Cost: • Kidney Txp: $ 60,000 • Islet cells 53,000 • Panc Txp alone 105,000 • SPK (K-P) 130,000 • Each year on dialysis: $27,000 • LOS for uncomplicated Kidney: • 5-7 days
Typical Kidney Course Creat Days after Transplant
Delayed Graft Function Course Biologic agent used first 10-14 days Creat Days after Transplant
Rejection • Clinical Diagnosis: • Hypertension • Increased Creatinine • Decreased urine output • Biopsy findings: • Tubulitis – usual Vasculitis - bad • Interstitial infiltration • Fixing of C 4 d
Rejection Biopsy findings Cellular Rejection Normal
Rejection • Differential Diagnosis • Not all ARF is rejection! • Drug toxicity • Ureter complication • Renal Artery Stenosis • Contrast, Aminoglycoside toxicity • Tubulo-interstitial Nephritis • Pre or Post renal causes • Recurrent disease (late)
Pattern of Acute Renal Failureafter Transplant Relative frequency Month after transplant
Rejection • 4 Types: • Hyperacute (preformed antibody) • Screened for with Lymphocyte crossmatch • Immediate/on the OR table • Rare due to testing • ADCC • Antibody dependent cellular cytotoxicity • 1-4 days post op • Rare occurance.
Rejection • 4 Types: • Acute • Most common • Due to Antigen presentation to an awakened immune system • Cellular or Vascular • Delayed Type or Chronic Rejection • Must be differentiated from drug nephrotoxicity
Rejection and Complement • Circulating Proteins in blood: • #1 Albumin • #2 Immunoglobulin • #3 Complement, esp C 3. • Triggers of Complement fixation • Ischemia reperfusion injury (IP - 10) • Brain injury in donor • Dialysis after transplant • Infection
Basic Immunology • Antigen presenting cells • Macrophages • Mesangial cells • Dendritic/Kupfer cells • Reticuloendothelial system (RES) • Endothelial cells and others once injured • D antigen expression
Basic Immunology • Cell mediated Immunity • Antigens: • Viruses, fungi, parasites, intracellular organisms • T cell lymphocytes • Cytotoxic • Directly attack and kill APC, Organism usually • Helper/ inducer cells • Recruit more immune cells to respond • IL-1 and IL-2 • Suppressor cells • Feedback to modulate immune response • Important for tolerance.
Basic Immunology • Humoral / Neutrophil system • Parallel to Cell mediated system • Antigens: • Usually bacterial cell polysaccharide • Antibodies • Produced by B lymphocytes • May be specific or nonspecific • IgG, IgM, others
Basic Immunology • Humoral / Neutrophil system • Immune complex formation Occurs when Antigen fixed by antibody Specificity of ab for ag determines size and solubility of Immune complex formed • Immune complex fixes complement • Complement activation increases clearance of I-C by spleen, etc • C3b chemotactic factor for PMN’s • PMN’s attack with lysozyme
Basic Immunology Antigen Presenting Cell Antigen plus HLA, coreceptors Humoral Cell Mediated T lymphocytes B cell Fc receptor comp C3b Cytotoxic Helper Suppressor Memory Pmn’s
Immunology of Rejection • HLA A and B are constitutive antigens • HLA D is inducible antigen • Infection, ischemia induce D antigen expression • D antigen expression leads to vascular rejection which is worst type • How does Bactrim SS MWF help?
Immunology of Rejection • HLA A and B are constitutive antigens • HLA D is inducible antigen • Infection, ischemia induce D antigen expression • D antigen expression leads to vascular rejection which is worst type • Bactrim SS MWF reduces bacteriuria
Immunology of Rejection • HLA A and B are constitutive antigens • HLA D is inducible antigen • Infection, ischemia induce D antigen expression • D antigen expression leads to vascular rejection which is worst type • Bactrim SS MWF reduces bacteriuria • What is Acyclovir used for after Txp?
Immunology of Rejection • HLA A and B are constitutive antigens • HLA D is inducible antigen • Infection, ischemia induce D antigen expression • D antigen expression leads to vascular rejection which is worst type • Bactrim SS MWF reduces bacteriuria • Acyclovir reduces shedding of Herpes Simplex virus in urine
Induction Immunosuppression • Biological Agents • Steroid use vs steroid sparing • Cellcept used in place of Imuran • Calcineurin Inhibitors / Sirolimus
Induction Immunosuppression • Biological Agents • OKT-3 rarely used • Thymoglobulin (rabbit) • ATG (polyclonal) • Basiliximab (Simulect) Chimeric • Anti CD 25/ anti IL-2 receptor monoclonal • Daclizumab (Zenapax) Humanized • Anti CD 25 Monoclonal
Induction Immunosuppression • Biological Agents • Expensive, complex to use • Use in high risk patients: • High PRA • Second transplant • African American recipient • Delayed Graft function
Induction Immunosuppression • Biological Agents • Basiliximab and Daclizumab • Anti CD 25 monoclonals • Do not deplete lymphocytes • Will not stop ongoing rejection • Other immunosuppression (CNI, steroid, MMF) should continue during use • OKT-3, ATG • Deplete lymphocytes, stop rejection, • reduce or withhold other immunosuppression while in use
Induction Immunosuppression • New Biological Agents coming soon: • CTL4 Ig • stimulates CTL4 coreceptor on T cell which leads to • Decreased activation • Apoptosis of the activated cell line • LEA 29 Y • a second generation CTL4 Ig
Regulation of T-Cell Activation IL-2 APC CD 40 CD 80/86 CD 25 CTL4 T-Cell Negative stimulatory Positive stimulation IL -2 Receptor
Induction Immunosuppression • Biological Agents recommendations • Low risk patient: • IL-2 receptor antibody, consider steroid sparing regimen • High Risk patient • Thymoglobulin plus 3 drug regimen • CNI, Steroids, MMF
Maintenance Immunosuppression • Categories of Agents: • Steroids • Calcineurin Inhibitors • Intracellular signal modifiers • Cyclosporine, Tacrolimus, Prograf • Adjuvant Agents • Interfere with cell cycling • Sirolimus, Rapamicin • Cellcept (MMF) • Imuran (azothioprine)
Where the drugs work • Steroids: • Toxic to lymphocytes • Stops rejection • Inhibits release of IL-1 and IL-2 • Inhibits chemotaxis
Where the drugs work • Cyclosporin A, Tacrilimus • Neoral, Prograf • Calcineurin Inhibitors (CNI) • Multiple effects on proliferating immune cells • Inhibits m-RNA producing IL-2 • Negligible effect on pre-sensitized cells • Does not stop ongoing rejection