Download
1 / 47
480 likes | 802 Vues
History, signs and symptoms of Hypertension. Dr. Ali-Akbar Tavassoli. Definition and classification of BP levels (mmHg). Source of Errors of BP Measurement. White-coat hypertension Physician measurement higher than BP taken by patients, nurses, technicians and home measurements

E N D
History, signs and symptoms of Hypertension Dr. Ali-Akbar Tavassoli
Source of Errors of BP Measurement • White-coat hypertension • Physician measurement higher than BP taken by patients, nurses, technicians and home measurements • 24 ambulatory BP monitoring may be helpful resolve this issue • Night dip
Source of Errors of BP Measurement (cont.) • Auscultatory Gap: • A period of silence after phase I and reappearing of Korotkoff sounds that causes missing phase II • This period is usually short but may be over 40mmHg • May be seen in elderly, fat arm, inflation too slow or inadequate, low intensity of Korotkoff sounds and venous congestion of upper extremity
Source of Errors of BP Measurement (cont.) • Auscultatory gap solution: • Rapid and adequate inflation (SBP estimated by palpation method first) • Increase the intensity of Korotkoff sounds by some maneuvered • Rapid inflation • Hold arm straight up during the inflation • Open and close fist 10 times during the inflation • 2nd measurement at least 1-2 minutes after the 1st
Source of Errors of BP Measurement (cont.) • Pseudohypotension: • Seen in patients with low cardiac output and shock state • High peripheral vascular resistance tightens the arteries to a point that generation of Korotkoff sounds is severely impaired and the sounds are too weak for accurate measurements of SBP or DBP and may lead to gross underestimation of BP
Psudo-hypertension • Occurs in elderly patients who have rigid arteries and should be suspected in elderly patients with high BP and no evidence of target organ damage • Osler’s maneuver may be beneficial • In elderly patients auscultatory gap is more frequent
Orthostatic Hypotension • A fall in SBP more the 20mmHg or DBP more 10mmHg in response to moving from supine position to a standing position within 3 minutes • Normally in erect position: • DBP never drops or rises slightly • SBP may decrease slightly • Mean BP doesn’t drops more a few mmHg • HR increases (except in neuropathy or using heart rate-slowing agent) • If HR increases, the 1st cause is hypovolemia
PulsusParadoxus • Normally SBP decreases in inspiration • if inspiratory decreases > 10mmHg, we call it PulsusParadoxus! • Major causes: • Pericardial tamponade • Status asthmaticus and obstructive lung disease
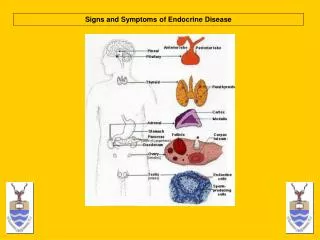
Diagnostic evaluation: medical and physical examination • Family and clinical history • 1. Duration and previous level of high BP • 2. indications of secondary HTN • 3. Risk factors • 4. Symptoms of organ damage • 5. Previous antihypertensive therapy (efficacy, adverse events) • 6. Personal, family, environmental factors
Physical examinations: • 1. Signs suggesting secondary HTN • 2. Signs of organ damage • 3. Evidence of visceral obesity
Risks influencing prognosis in patients with hypertension • Risk factors for cardiovascular disease • Levels of SBP and DBP • Age- men>55; women>65 • Smoking • Family history of premature cardiovascular disease • Abdominal obesity • Diabetes • CRP >= 1mg/dl
Subclinical target organ damage • Left ventricular hypertrophy • Ultrasound evidence of arterial wall thickening or atherosclerotic plaque • Estimated GFR =< 60 ml/min/1.73 m3 • Microalbuminuria
Clinical target organ damage • Cerebrovascular disease • Ischemic stroke • Cerebral hemorrhage • TIA • Heart disease • MI or ACS • Angina • Coronary revascularization • CHF • Renal disease • Diabetic nephropathy • Chronic kidney disease • Proteniuria>300 mg/24 h • Peripheral arterial disease • Advanced retinopathy • Papiledema
Identifiable causes of hypertension • Sleep apnea • Drug induced or related causes (see table 9) • Chronic kidney disease • Primary aldostronism • Renovascular disease • Chronic steroid therapy and Cushing’s syndrome • Pheochromocytoma • Coarcation of the Aorta • Thyroid or parathyroid diseases
Drug-induced HTN • Non-steroidal antiinflammatory drugs; cycloxygenase 2 inhibitors • Cocaine, amphetamines, other illicit drugs • Sympathomimmetics (decongestant, anorectics) • Oral contraceptives • Adrenal steroids • Cyclosporine and Tacrolimus • Erythropoietin • Licorice (including some chewing tobacco) • Selected over-the-counter dietary supplements and medicines (e.g, ephedra, mahung, bitter orange)
Associated conditions • Obesity • Excess alcohol intake
HTN and tachycardia • Hyperthyroidism • Pheochromocytoma • Hyperkinetic syndrome • Anxiety
HTN and bradycardia • B-Blocker • Heart block • Hypothyroidism • Increased intracranial pressure (Cushing reflex) as ICH, Tumors, Meningitis…
HTN with nocturia • Renal disease • Hyperparathyroidism • Hyperaldostronism • Sleep-disordered breathing
HTN and postural hypotension • Pheochromocytoma • Renovascular HTN (decreased diastolic pressure) • Drugs (alpha-blocker, antidepressant) • Autonomic failure • Porphyria
HTN with café au lait spots • Pheochromocytoma • Renovascular HTN (Fibromascular) • Abdominal Coarcation
HTN and palpable abdominal mass • Polycystic kidney disease • Renal tumors • Hydronephrosis • Rarely pheochromocytoma
HTN and attacks of Paroxysms • Pheochromocytoma • Rebound HTN after abrupt cessation of clonidine and other antihypertensive drugs • Hypertensive crises with MAO inhibitors • Acute pulmonary edema • Hypoglycemia • Anxiety and panic attacks • Spinal cord transection (during bladder distension or muscle spasm) • Menopausal symptoms
HTN with hyperglycemia • Diabetes • Pheochromocytoma • Acromegaly • Cushing syndrome
HTN and unprovoked hypokalemia • Primary hyperaldostronism • Renovascular HTN • Malignant HTN • Cushing syndrome • Liddle syndrome
HTN with hypercalcemia • Hyperparathyroidism • Pheochromocytoma • During chronic thiazide therapy in patients with pre-existing hyperparathyroidism o r vitamin D-treated hypoparathyroidism • MEN and other disease such as sarcoidosis, multiple myeloma
Features of clinical clues for secondary HTN • Age on onset: <25 or > 50 • Recent HTN with rapid progression • Malignant HTN without history of chronic HTN • Symptomatic HTN • History of hematuria, flank pain, back trauma, surgery and abdominal radiation • Palpable kidney • HTN with unprovoked hypokalemia, hypercalcemia, hyperglycemia, serum cr>1.5, anemia, weight loss • Abdominal bruit • HTN with pulse pressure or unequal pulses of lower and upper extremities
Age • Age is an important factor in hypertensive patients • New born infants (always secondary hypertension) • Renovascular, thrombosis or renalarterystenosis (RAS) • Coarctation of aorta (COA) • Congenital renal malformation • Broncopulmonary dysplasia • Pre school (almost always secondary) • Renal (pronchymal or vascular) • After 10 years • Renal disease • Essential hyper tension (strongly with family history and obesity)
Secondary HTN Coarcation of Aorta • Absent or reduced pulses in the lower extremities • Pulsation in neck • Palpable pulsations over intercostal arteries in the posterior thorax • Bruits over the intercostal arteries • Rib notching on CXR • Cold feet • Pain in legs with exercise
Sings or symptoms suggesting Renovascular hypertension • Age <30 or >50 • Young female (fibromuscular) or old men (atherosclerosis) • Sever resistant HTN • Abrupt onset of HTN • Abdominal continuous or prolonged high-pitched systolic bruit • Symptoms of atherosclerosis elsewhere • Orthostatic drop of DBP • Recurrent pulmonary edema especially with good left ventricular function • Significant azotemia in response to ACEI
Sings or symptoms suggesting Renovascular hypertension (cont.) • Small unilateral kidney • HTN and unexplained impairment in renal function • Arteritis (Takayasu’s-PAN) • Rejected kidney • Aortic dissection • Retroperitoneal fibrosis • Significant kidney ptosis on IVP or orthostatic HTN • Lab test: hypokalemia, proteniuria, increased renin levels • Azotemia in the elderly patient with atherosclerosis elsewhere
Post-transplant Hypertension • Very Frequent • Causes: • Retained native kidney • Recurrent disease in allograft • Acute or chronic rejection • Donor factor • Transplant renal artery stenosis • Immunosuppressive drugs (steroid, cyclosporine, etc)
Pheochromocytoma Signs and symptoms “10 H’s” • HTN (>90%) • Hypotension (orthostatic) • HTN crises (50%) • History of labile blood pressure • Headache • Heart consciousness (palpitation) • Heat intolerance • Hyperhydrosis (sweating) • Hypermetabolism • Hyperglycemia
Pheochromocytoma HTN+ “10 P’s” • Pain • Paroxysm (50%) • Postural hypotension • Pallor • Polar (coldness) • Perspiration • Pressor response to antihypertensive agents (alpha-blockers, vasodilators, TCA or during induction of anesthesia) • Pupils dilatation • Psychological disorders *symptoms and signs may occur without HTN crises
Conditions that may simulate Pheochromocytoma • Hyperdynamic labile HTN • Paroxysmal tachycardia • Angina, Coronary insufficiency • Acute pulmonary edema • Ecclampsia • HTN crises during or after surgery • HTN crises with MAO inhibitors • Rebound HTN after abrupt cessation of clonidine or other antihypertensives
Conditions that may simulate Pheochromocytoma (cont.) • Psychoneurological • Anxiety with hyperventialtion • Panic attacks • Migraine and cluster headaches • Brain tumor • Basilar artery aneurysm • Stroke • Diencephalic seizure • Porphyria • Lead poisoning • Familial dysautonomia • Acrodynia • Autonomic hyperreflexia as with quardiplegia • Baroreflex failure • Fatal familial insomnia
HTN Cause • Endocrinological • Menopausal symptoms • Thyrotoxicosis • Hypothyroidism • Diabetes Mellitus • Hypoglycemia • Carcinoid • Mastocytosis • Factitious: ingestion of sympathomimetics
Primary hyperaldostronismClinical and lab clues • HTN • Bilateral headache • Proximal muscle weakness of extremities and paresthesia • Lack of edema • Nocturia and polyuria • Unprovoked hypokalemia (<3.5 meq/L) • Failure to normalized serum K values within 4 weeks off diuretics • Sever hypokalemia after initiation of diuretic therapy • Difficulty maintaining normal serum K values despite concomitant use of oral K or K-sparing agents with conventional dose of diuretics • 24-h urinary K (>30 meq/L) despite low serum K (<3meq/L)
The clinical features of preeclampsia • HTN • Epigastric/right upper quadrant pain • Fetal growth restriction • Convulsion • Headache • Coma • ICH • Visual disturbance • Pulmonary edema • Bleeding from venipuncture sites • Proteinuria • ARF • Placental abruption • Hyperreflexia • Edema • Clonus
HTN patients require additional diagnostic testing • -Age, history, examination, severity of HTN, or initial laboratory findings suggest secondary HTN • Resistant HTN on maximal dosage of at least 3 appropriate anti-hypertensive drugs • Previous good BP control with acute unexplained exacerbation • HTN associated with grade 3 or 4 retinopathy • New-onset HTN after age 60 • Suspected new or worsening target organ damage
Complications of hypertension • 1-Hypertensive • Accelerated-malignant hypertension (grades III and IV retinopathy) • Encephalopathy • Cerebral hemorrhage • LVH • CHF • Renal insufficiency • Aortic dissection • 2-Atherosclerotic