Download
1 / 28
280 likes | 333 Vues
Learn about hypopituitarism, its causes, clinical features, diagnosis, and treatment. Explore the physiology of pituitary hormones and investigations required for diagnosis.

E N D
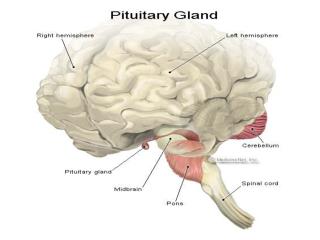
Syndromes of Pituitary Hormone Deficiency Dr Mohamed Abdel WahabEzzat Lecturer of Internal Medicine and Cardiology Faculty of Medicine Sohag University
Hypopituitarism; Anterior Pituitary Hormone deficiency • Caused by either deficiency of hypothalamic releasing hormones or of pituitary trophic hormones. • Deficiency is either selective or multiple. • Isolated deficiency is rare, some of which may be congenital, autoimmune or idiopathic in nature. • Multiple deficiencies may result from a tumor, surgery, radiotherapy or other destructive lesions. Rarely due to a congenital defect. • Panhypopituitarism refers to deficiency of all anterior pituitary function.
Congenital Isolated deficiency; e.g Kallman’s syndrome Multiple; gene mutation (Pit-1 deficiency) Neoplastic Pituitary or hypothalamic tumors Craniopharyngeoma Secondary deposits Autoimmune; - Pituitary antibodies Vascular Sheehan’s syndrome. Pituitary apoplexy Traumatic Surgery Head injury Infective Meningitis Encephalitis Others Radiotherapy chemotherapy Causes of Hypopituitarism
Clinical Features of Hypopituitarism • With progressive lesions of the pituitary there is a characteristic sequence of loss of pituitary hormones; • GH is often the earliest lethargy, weakness, increased fat mass. • Next gonadotrophins oligomenorrhea or amenorrhea in females, decrease in pubic and axillary hairs,….. • Hyperprolactenemia rather than prolactin deficiecy
Clinical Features of Hypopituitarism • Next, ACTH deficiency symptoms of cortisol deficiency, however, in contrast to Addison’s disease: - Aldosterone secretion is not affected, thus serum K+ level is maintained normal. - Pallor rather than hyperpigmentation because of lack of stimulation of melanocytes . • Finally, TSH is lost secondary hypothyroidism. • Untreated severe cases may results in coma due to hypoglycemia, water intoxication or hypothermia
Physiology Positive regulation Negative regulation Hypothalamus GnRH TRH Dopamine GHRH Somatostatin CRH ADH Oxytocin Ant pituitary LH&FSH TSH Prolactin GH β-LPH ACTH Post pituitary Target organs Gonads Thyroid Breast Tissues Melanocytes Adrenals Nephrons breast uterus Target hormones Sex T3 IGF-1 Cortisol Hormones T4
Investigations of Hypopituitarism • Each axis requires separate investigation. • Stimulation tests are often required; • GH; - measurement 1 h after going to sleep, frequent sampling during sleep. - post exercise measurement. - Insulin-induced hypoglycemia: only in specialized centers, basal cortisol must be> 100nmol/l, normal free T4 level. overnight fast, IV insuline 0.15 unit/kg, repeated measurement of glucose, ACTH and growth hormone.
Investigations of Hypopituitarism • ACTH; - ACTH stimulation test; 250µg tetracosactrin (Synacthen) Im, sampling of blood for plasma cortisol at 0 and 30 min. normally: cortisol rises to 550nmol/l. • TSH; - random thyroxin level + TSH • Gonadotrophins - in males; random S. testosterone. - ask about menstrual cycles or measure random LH and FSH in post menopausal women.
Treatment of hypopituitarism • Treatment of the cause. • Adequate replacement therapy; • Cortisol; orally as hydrocortisone start with 15 mg at the morning, 5 mg at evening. • Thyroxin; maintain S. thyroxin at the upper level of normal; start by 0.1-0.15 mg once daily. TSH measuremen is unhelpful. N.B.: treatment with steroid should start before thyroid replacement therapy.
Treatment of hypopituitarism • Gonadotrophins; - males; testosterone injections weekly or twice daily orally. - females; cyclic estrogen and progesterone. - when fertility is desired; gonadal stimulation by HCG or by pulsatile GnRH. • GH; mainly administered to young children to attain normal growth. In adults needed to improve lethargy and other metabolic abnormalities. Start with 0.125iu/kg/week, increase gradually, monitor by s. IGF-1
GROWTH FAILURE: SHORT STATURE When children or their parents complain of short stature, particular attention should focus on: • intrauterine growth retardation, weight and gestation at birth • possible systemic disorders - any system, but especially small-bowel disease • evidence of skeletal, chromosomal or other congenital abnormalities • endocrine status - particularly thyroid • dietary intake and use of drugs, especially steroids for asthma • emotional, psychological, family and school problems.
Causes of short stature • Constitutional delay • Familial short stature • Gh insufficiency • Primary hypothyroidism • Small bowel disease
Investigations • Systemic disease having been excluded, the following should be undertaken: • Thyroid function tests - serum TSH and free T4 to exclude hypothyroidism.
Investigations • GH status. Basal levels are of little value, though urinary GH measurements may prove to be of some value in screening. • Dynamic tests include the GH response to insulin. Test should only be performed in centers experienced in their use and interpretation.
Investigations • Assessment of bone age. Non-dominant hand and wrist X-rays allow assessment of bone age by comparison with standard charts.
Treatment • Systemic illness should be treated and primary hypothyroidism replaced with thyroxine. • For GH insufficiency, recombinant GH (somatropin) is given as nightly injections in doses of 0.17-0.35 mg/kg per week. • Treatment is expensive and should be supervised in expert centers.
Treatment • GH treatment in so -called 'short normal' children has not been shown to produce any worthwhile increase in final height.
Anti-Diuretic Hormone • Thirst axis • Thirst and water regulation are largely regulated by anti-diuretic hormone (ADH or vasopressin) which synthesized by the hypothalamus. • At normal conc. Kidneys are the predominant site of action of ADH via V2 receptors at the collecting tubules. • At high conc., it causes vasoconstriction via V1 receptors. • Its secretion is stimulated by increased osmolality, hypovolemia or hypotension and vise versa.
Disorders of Vasopressin (ADH) secretion or activity • Deficiency as a result of hypothalamic disease (cranial diabetes insipidus). • Inappropriate excess of ADH secretion. • Nephrogenic diabetes insipidus; the renal tubules are insensitive to vasopressin (receptor abnormality).
Diabetes Insipidus; Causes • Cranial D.I. • Familial; due toa genetic defect, e.g. DIDMOAD; rare, autosomal recessive. • Tumors; hypopthalamic or pituitary with suprasellar extension. • Traumatic ; head injury or post-surgical • Post-radiotherapy. • Infections; T.B, meningitis. • Vascular; Heamorrhage, thrrombosis, Sheehan’s syndrome. • Infiltrations; sarcoidosis, histiocytosis. • Idiopathic.
Diabetes Insipidus; Causes • Nephrogenic D.I. • Familial; e.g. Vasopressin-2 receptor gene defect (sex-linked recessive), or, defect in an ADH-sensitive water channel (aquaporin-2). • Metabolic abnormality; e.g. hypokalemia, hypercalcemia. • Renal disease; e.g. renal tubular acidosis. • Drugs; demeclocycline, glibenclamide lithium. • Heavy metal poisoning.
D. I.; Clinical features. • Polyuria, nocturia, compensatory polydypsia. • The patient may pass as much as 10-15 L of urine/ day. • Severe dehydration can occur if there is disturbance in the thirst mechanism or conscious level. • Differential diagnosis: • Primary polydpsia (hysterical) • Diabetes mellitus
D. I.; Investigations & Diagnosis • High 24 h urine volume (<2 L exclude diagnosis) • High or high normal plasma osmolality (>300mOsm/kg) with low urine osmolality (<660mOsm/kg). • Water deprivation test; monitor serum and urine osmolality, urine volume and body weight hourly for 8 hours. Proceed to desmopressin administration i.m. and monitor the response.
D. I.; Treatment • Desmopressin; synthrtic analogue of vasopressin is given intranasally as a spray 10-20 µg once or twice daily , orally as 200 µg three times daily or i.m. injection 2-4 µg. daily. Effective only in cranial type. • Alternative therapy; sensitization of the renal tubules to endogenous vasopressin by thiazide diuretics, carbamazipen or non-steroidal anti-inflammatory as indomethacin.
Syndrome of Inappropriate ADH secretion (SIADH) • Inappropriate secretion of ADH leads to retention of water and hyponatremia. • Causes; usually secondary to: • Tumors: small cell carcinoma of the lung, prostate, pancreas or lymphoma. • Pulmonary lesions; pneumonia, T.B. • CNS lesions; head injury, tumors, meningitis. • Drugs; as chrorpropamide, carbamazipen, phenothiazines.
Syndrome of Inappropriate ADH secretion (SIADH) • Diagnosis: • Dilutional hyponatremia. • Low plasma osmolality with inappropriate urine osmolality. • Urinary Na excretion > 30mmol/L. • Treatment: • Restriction of fluid intake (500-1000ml/day). • Demeclocycline 600-1200mg/day; causes reversible type of nephrogenic D. I.