Download
1 / 46
500 likes | 955 Vues
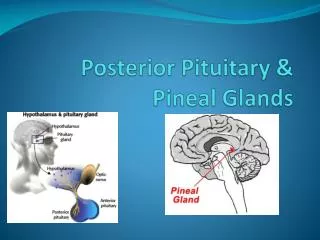
Diseases of Posterior Pituitary. Hasan AYDIN , MD Yeditepe University Medical Faculty Department of Endocrinology and Metabolism. Posterior Pituitary. Posterior p ituitary (n eurohypophysis ) I t is continuous with the brain

E N D
Diseases of Posterior Pituitary Hasan AYDIN, MD Yeditepe UniversityMedicalFaculty Department of EndocrinologyandMetabolism
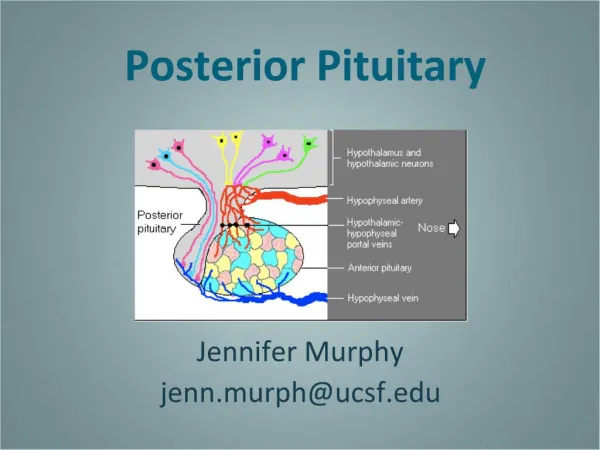
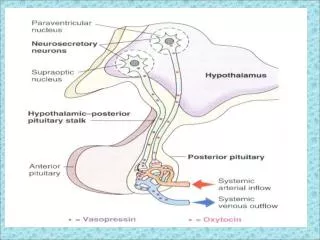
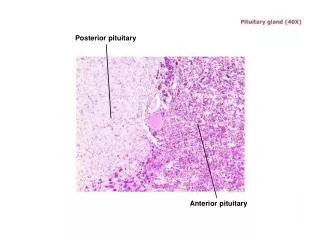
Posterior Pituitary Posterior pituitary (neurohypophysis) • It is continuous with the brain • Formed during embryonic development from an outgrowth of the inferior part of the brain in the area of the hypothalamus • Secretions of the posterior pituitary are considered asneurohormones
Antidiuretic Hormone (ADH) • Named so because it prevents the output of large amounts of urine • Constricts blood vessels and raises blood pressure when large amounts of urine are released • Its primary target tissue is the kidneys, where it promotes the retention of water, and reduces urine volume • Urine volume increases within minutes to a few hours in response to increased water intake, and decreases if water is not consumed.
Antidiuretic Hormone (ADH) • 1 % increase in osmolality (3 mOsm/kg H2O) stimulates ADH secretion. • Serum osmolality above 290 mOsm/kg H2O (N: 285 mOsm/kg H2O) stimulates thirst center. • The actions of ADH is mediated by G-protein coupled cell surface receptors V1, V2, V3
V1 Receptors • Located on • Vascular smooth muscle cells • Liver • Thrombocytes • Renal medulla, hypocampus, amygdala, hypothalamus and brain stem • When stimulated causes • Vasoconstriction • Glycogenolysis • Thrombocyte aggregation
V2Receptors • Found on renal distal tubular and collecting duct cells • V2 receptor gene is on short arm of X chromosome (Xq28). • Mutations cause congenital X-linked Nephrogenic DI
V3Receptors • Found on ACTH secreting cells of anterior hypophysis • Activation with ADH causes ACTH release
Regulationof ADH Secretion ADH Releaseisstimulated by: • A plasma osmolality >280 mOsm/l • A fall in plasma volume • Emotionalfactors & stress • Sleep • Otherfactors (nausea, hypoglycemia, hypoxia, acidosis)
Other ADH Stimulants • Cholinergic stimulation • Αlpha-adrenergic stimulation • Angiotensin II • Prostoglandin E • Opiates • Nicotine • Histamine • Ether • Phenobarbitone
ADH Secretion is Inhibited by: • Alcohol • Oropharengeal water reflex • β-adrenergic stimulants • Atrial natriuretic factors (ANF) • Phenytoin
Functionsof ADH • Primary Effect • Water reabsorbtion from the distal tubules and collecting ducts of the kidney • Mediated by V2 receptors through the activation of cAMP and formation of a spesific protein known as “AQUAPORIN”
Actions of ADH • During hypovolemia plasma levels of ADH maintain tissue perfusion • Via V2 stimulates synthesis and release of factor VIII & Von Willebrandfactor
Disorders/diseases resulting from dysfunction • Excess:Syndrome of Inappropriate ADH secretion (SIADH) • Deficiency:Diabetes Insipidus
DiabetesInsipidus • Syndrome of posterior pituitary hypofunction • S/S • Increased thirst - polydipsia • Increased urination - polyruia • Results from • ADH (Vasopression) deficiency, which prevents the kidneys from reabsorbing water • Inability to conserve water
Typesof Diabetes Insipitus • Cental Diabetes Insipidus • Nephrogenic DiabetesInsipidus • Dispogenic Diabetes Insipidus • Gestational Diabetes Insipidus
Central Diabetes Insipitus(Neurogenic DI) • Results from damage to the pituitary gland • Results in a deficiency of antidiuretic hormone (ADH).
Nephrogenic Diabetes Insipitus • Vasopressin-resistant. • Caused by insensitivity or inability of the kidneys to the effect of ADH. • Can be caused by • Certain drugs such as lithium • Blockade of the ureters • Genetic disorders (Mutations in the aquaporin-2 gene )
Dipsogenic DI (primarypolydipsia) • Occurs when vasopressin is suppressed by excessive intake of fluids • Most often caused by an abnormality in the part of the brain that regulates thirst • Primary polydipsia is due not to abnormal thirst but to psychosomatic causes
GestationalDI • Occurs during pregnancy • An enzyme made by the placenta destroys ADH in the mother • DI often disappear 4 to 6 weeks after delivery • Oftenrecur with subsequent pregnancies
Causes of Central Diabetes Insipidus • Hypophysectomy, complete or partial • Surgery to remove suprasellar tumors • Idiopathic • Familial • Tumors and cysts (intra- and suprasellar) • Histiocytosis • Granulomas • Infections • Interruption of blood supply • Autoimmune
Causes of Nephrogenic Diabetes Insipidus • Chronic renal disease • Hypokalemia • Protein starvation • Hypercalcemia • Sickle cell anemia • Sjögren's syndrome • Drugs, eg, lithium, fluoride, methoxyflurane anesthesia, demeclocycline, colchicine, foscarnet, cidofovir • Congenital defect • Familial
Clinical Features • Poliuria, polydipsia & thirst • Nocturiaor nocturnal enuresis • Hypernatremic dehydration • Anorexia, constipation • Hyperthermia and lack of sweating • Symptoms of underlying cause
Diagnostic Work-up • Document presence of polyuria (usually 4-5 L/24 hours) • Measurement of plasma and urine osmolality • In DI • Plasma osmolality >295 mOsmol/l • Urine osmolality 50-150 mOsmol/l
Water Deprivation Test • Useful in patients with partial ADH deficiency • Differentiate DI from primary polydipsia
Water Deprivation Test • Should be done in the morning under supervision • Weigh hourly and measure plasma and urine osmolality every 2 hours • In pts with DI plasma but not urine osmolality rises, U/P osm ratio < 1.5 • Testing can proceed if urinary osmolality stabilized for 3 samples and 3% wt loss is noted • At the end of the test ADH given (20 mg DDAVP intranasallyor 2 mg im) and fluid intake allowed • Concentration of dilute urine confirms central DI and failure suggests nephrogenic causes
Differential Diagnosis • Psychogenic polidipsia • Medullary cystic disease • Drugs (Lithium, diuretics) • Osmotic diuresis (DM) • Hypercalcemia, hypokalemia • Postobstructive diuresis (pyelonefritis, renal tubular acidosis, sickle cell anemia) • Hyperthyroidism
Treatment • Desmopressin (DDAVP): • A synthetic analogue • Longer duration of action (8-10 h vs 2-3 h) • More potent • ADH activity 3000 x greater than pressor activity • Usually given intranasally but sc and oral administration possible
Treatmentof Nephrogenic DI • Provision of adequate fluids and calorie • Low sodium diet • Diuretics • High dose of DDAVP • Correction of underlying cause • Drugs (Indomethacin,Chlorprooramide, Clofibrate & Carbamazepine)
SyndromeofInapproriateSecretion of ADH (Posterior Pituitary Hypersecretion)
SIADH occurs: • When there is too much vasopression (ADH) with inappropriate water retention and decreased blood Na levels
Syndrome of Inappropriate Antidiuretic Hormone Secretion - SIADH • Results from • Inability to produce & secrete dilute urine • Water retention • Increased extra cellular fluid volume • Hyponatremia • Diseases that affect the hypothalamus
Etiology • 1.Central Nervous System Diseases • Menengitis, Ensephalitis, Abcess, Trauma, • Hypoxic ischemic state, Tumor, • Guillain Barre Syndrome, • Ventriculo- atrial shant obstruction, • Acute intermittant porfiria, • Sinus thrombosis, • Hemorrhagia (Intracerebral, subarachnoid).
2. Respiratory system diseases Pneumonia, aspergillosis, tbc, Positive pressure ventilation, Pneumotorax, atelectasia, astma, cystic fibrosis, 3. Malignancy, Thymoma, Lymphoma, Ewing sarcoma, Duedonum, Pancreas, Ureter, Prostate, Baldder and Bronchogenic carcinoma, 4. Drugs eg. vincristin, 5. Myxedema 6. Idiopathic.
SIADH • Increased secretion of AVPcauses euvolemic hyponatremia. This causes abnormal thirst and intake of excess water leading to accumulation of water and at the enddilutional hyponatremia. • As a result, • serum Nadecreased. • urinary excreation of Naincreased. • urine density and osmolalityincreased.
Clinical Findings • Anorexia, apathy, confusion, headache, weakness, cramps in abdominal and extremity muscles , nausea, vomiting, abdominal floating • Neurological signs include slowness in DTR, pathological reflexes, in severe cases convulsions and coma.
Dx of SIADH • The following criteria should be fulfilled before a diagnosis of SIADH can be made: • persistent excretion of concentrated urine with no reason for ADH release • normal renal and adrenal function • no edema or hypovolaemia should be present • the urine osmolarity should be greater than the serum osmolarity
Lab Assessment in SIADH • Elevated urine sodium levels and specific gravityreflect anincreased concentration of the urine • Serum sodium levels are decreased,often as low as 110 mEq/L(normal serum sodium 135-145 mEq/L) due toextracellular volume expansionandincreased Na excretion • Fluid retentioncauses changes in bothplasma and urine osmolality • Plasma osmolality is decreased, and theurine is hyperosmolarin relation to the plasma
SIADH Treatment • Water Restrictionis the cornerstone of treatment • Decreased water intake allows serum sodium level to rise normally. • The maximum amount of water that pt with SIADH are allowed to drink is just slightly more that the amount of urine they produce • Pt must have regular serum sodium measurements to ensure that the water restriction has been effective • Dehydration-The most concerning potential side effect from treatment is dehydration.
SIADH Treatment • Restrict fluid intake (800-1000 cc/day) • Daily weight Strict I & O • Monitor urine specific gravity • 0.9 NS infusion(to raise the serum Na level if water intoxication is severe) • Monitor for hyponatremia • Furosemide may be admin to block circulatory overload • Drugs-demeclocyclin HCL & lithium-may be admin to block renal response to ADH, intereferes with action of ADH • Drugs - Phenytoin - inhibits ADH release • Surgery & Chemo -to remove or destroy neoplasms that may be the underlying cause of this syndrome
SIADH Treatment • Demeclocycline (Declomycin) • Lithium • Used for: • Excess secretion of ADH or SIADH • Action: • Inhibits ADH action in kidney • Blocks renal response to ADH, interferes with action of ADH • Therapeutic outcome: • Decreased urine specific gravity