S troke
Jody L. Zak MS, PA-C. S troke. 1. What are the 2 types of Stroke? 2. Most common type of Stroke? 3 . I nitial workup includes (#1 priority)? 4 . What is the most common scale used when assessing possible Stroke patients?

S troke
E N D
Presentation Transcript
Jody L. Zak MS, PA-C Stroke
1. What are the 2 types of Stroke? 2. Most common type of Stroke? 3. Initial workup includes (#1 priority)? 4. What is the most common scale used when assessing possible Stroke patients? 5. What is the name of the clot-busting agent used to treat ischemic strokes? Time frame you must use this treatment? Stroke Pre-Test
Stroke is the interruption to blood supply of the Central Nervous System. Stroke is the third leading cause of death in the US Stroke affects approximately 15,000,000 people per year (new & recurrent) Every 40 sec someone in the US has a CVA In the US, approx. one out of fifteen deaths result from a CVA On average 1 person dies every 3-4 minutes from a CVA Some statistics from the American Stroke Association
Estimated cost (indirect and direct) of stroke in 2007 is 62.7 billion. ~80% of strokes are ischemic. Hemorrhagic make up the rest Statistics Continued
“Focal ischemic cerebral neurologic deficits that last for <24 hours (usually 1-2 hours)” 30% of stroke patients have h/o TIAs Symptoms lasting “a few seconds” is probably not a TIA TIA is a CLINICAL SYNDROME and Does NOT refer to a radiographic finding Transient ischemic attacks (TIA)
Unilateral weakness of one or two extremities Clumsiness Sudden difficulty speaking Numbness/tingle in an extremity Vision changes (loss in one eye or visual field), Amaurosis Fugax does usually not occur at the same time TIA Symptoms
Amaurosis is the Greek word for darkening, dark, or obscure Fugax means fugitive or fleeing Sudden loss of vision in one eye Temporary disruption of blood flow to retinal artery Described as curtain coming down over eye Emboli from carotid artery AmaurosisFugax
Similar to that of a CVA. Labs: CBC, fasting lipid profile, lytes CT head without contrast TTE/TEE Carotid Dopplers Consider MRI if CT negative Workup
A-V Malformations (AVM) Focal seizures Hyper/hypoglycemia Meniere’s Dz (if symptom is vertigo) Migraine Neoplasm Differential Diagnosis TIA
Antiplatelet agents: ASA, plavix, aggrenox Treatment of TIA
After a TIA, highest risk period is the 1st 30 days (primarily first 48 hours) then declines People with a TIA have a 10 year CVA risk of approx. 18.8% Risk for future CVA (cerebrovascular accident)
Increased age (Elderly > middle age) Heredity Race/ethnicity (A.A. > Hispanic > white) Sex (male > female in all age groups) Family hx of premature vascular dz Risk factors-Stroke/CVA
Alcoholism/illicit drug use Heart dz/A-fib/MI/CHF with LVF <25% Tobacco use DM HTN Obesity OCP Hyperlipidemia Modifiable risk factors
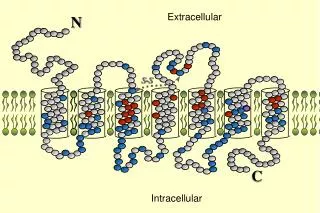
Common causes of arterial occlusion involving the major cerebral arteries are as follows: Embolization (particles from elsewhere) most come from atherosclerotic (hardening of the artery/fat/cholesterol) narrowing at the bifurcation of the common carotid artery Cardiac sources Thrombosis Local obstruction Blockage due to damage to the arterial wall (lacunar) Blockage of a single artery can often be compensated for by other arteries in the blood vessel network, call collaterals Pathophysiology
ATRIAL FIBRILLATION Recent MI Dilated cardiomyopathy Hypokinesis Mural or Intraventricular thrombus Atrial septal defect/ patent foramen ovale Atrial Myxoma Cardiac sources of embolic CVA
Rheumatic mitral stenosis Valvular abnormalities Mitral valve prolapse Endocarditis Calcific aortic stenosis Cardiac sources of embolic CVA
Atherosclerosis of aortic arch Intra/extracranial large artery disease Small artery disease Causes of ischemic CVA
Arterial dissection Vasospasm Marfan’s syndrome **Hyperhomocysteinemia Amyloid angiopathy Vasculopathies (noninflammatory)
Polyarteritis nodosa Wegener’s granulomatosis SLE Scleroderma Sjogren’s syndrome Temporal arteritis Sarcoidosis Drug-induced vasculitis Inflammatory
Brain tumor SDH Seizure with postictal paralysis (Todd’s Paralysis) Hypoglycemia Migraine Brain abscess encephalitis Differential Diagnosis
Based on location of stroke • Anterior Circulation • Supplied by the Carotid arteries • Posterior Circulation • Supplied by the Vertebral and Basilar arteries • Circle of Willis Symptoms
This the most commonly affected vessel by a CVA. There are 4 segments to the MCA. The MCA bifurcates. The superior branch supplies the prefrontal cortex. The inferior branch supplies the temporal regions. Middle Cerebral Artery (MCA) Distribution
Occlusion of the main trunk: • Contralateral hemiplegia, hemisensory loss • Face/arm> leg • eye deviation toward the side of the lesion • Homonymous hemianopsia; bil symmetric loss of vision in half of the visual fields. • Aphasia; expressive (Broca’s) if on dominant side Physical Exam Findings in MCA Stroke
Superior division infarcts cause contralateral upper extremity and face weakness. The lower extremity is usually not affected. Inferior division infarcts can cause quadrantanopsia or homonymous hemianopsia or visual neglect. Physical Exam Findings in MCA Stroke
Right hemisphere (nondominant) Neglect Confusion Confabulation “honest lying” Physical Exam Findings in MCA Stroke
Uncommon, accounting for approximately 2% of all cases supply the anterior limb of the internal capsule, the inferior head of the caudate nucleus, and the anterior part of the globus pallidus Anterior Cerebral Artery (ACA) Stroke
Contralateral weakness of lower extremity There can also be weakness of the contralateral arm especially proximally Contralateral hemisensory loss Because ACA supplies frontal lobes, there can be frontal lobe signs such as abulia (lack of initiative), confusion, and other behavioral issues Urinary incontinence is not uncommon Anterior Cerebral Artery (ACA) Stroke
Accounts for approximately 5% of CVA Supplies midbrain, the subthalamic nucleus, the basal nucleus, the thalamus, the mesial inferior temporal lobe, and the occipital and occipitoparietal cortices. Posterior Cerebral Artery Stroke
Most patients complain of vision problems, “bumping into things”, lightheaded/dizziness, and parasthesias Contralateral hemiparesis->damage to verebral peduncle Hemisensory loss->thalamus Amnesia->medial temporal lobe Physical Exam findings in PCA Stroke
Can have Thalamic Syndrome which is characterized by contalateralhemisensory impairment in which there is usually spontaneous pain. Visual field deficits are most common symptom in unilateral PCA infarcts. Homonymous hemianopsia with macular sparing (because of collateral vascular supply from posterior MCA) Physical Exam findings in PCA Stroke
Supplies Base of Brain; medulla, cerebellum, pons, midbrain, thalamus, and occipital cortex Vertebral arteries come off the subclavian arteries. They enter the skull through the foramen magnum and merge to form the basilar artery. Both vertebral arteries give off posterior inferior cerebellar artery (PICA) May be clinically silent if occlusion is distal to origin of Anterior spinal and PICAs. Vertebrobasilarischemia
Ataxia Dysarthria/dysphagia, CN signs Bilateral sensory or motor sx Nausea/vomiting/vertigo if vestibular system is affected Gaze abnormalities, i.e.diplopia Changes in mental status/level of consciousness Vertebrobasilar infarct
WallenburgSyndrome: (lateral medulla) is caused by vertebral infarct but can be caused by PICA as well. Pt’s present with N/V and vertigo, ipsilateralataxia and Horner’s syndrome (ptosis, miosis, anhidrosis), facial pain, contralateral pain and temperature loss. Weber’s: midbrain lesion, CNIII palsy with contralateral weakness Claude: lesion of the red nucleus, CN III palsy with contralateral rubal tremor. Common vertebrobasilar syndromes
BA occlusions usually produce drastic deficits/fatal. Locked in syndrome (medulla sparing); patients are quadriplegic with vertical eye movements. Another vertebrobasilarsyndrome
Anterior/Carotid Circulation • Hemispheric • Aphasia, Transient monocular blindness (AF), Hemiparesis, Hemisensory deficit • Posterior/Vertebrobasilar • Brainstem/cerebellar • Bil vision loss, diplopia, nystagmus • Ataxia, vertigo, syncope, dysarthria, vomiting Summary
Most common lesions found in the brain stem, cerebral artery. Small lesions (< 5mm diameter)found most commonly in deep cortical sites (basal ganglia) and brainstem(pons and thalamus) Associated with HTN (poorly controlled) and DM 80% of Lacunar infarcts go unnoticed Not always picked up on CT scan (small infarcts) in deep cortical sites (basal ganglia) and brainstem Most Common syndrome: Pure motor hemiparesis pure sensory hemiparasthesias dysarthria-clumsy hand syndrome Lacunar infarcts
Caused by atherosclerosis Prognosis generally good Infarct may worsen over first 24-36 hours CT often normal Tmt: aspirin, control risk factors (HTN, DM) Lacunar cont.
Disability caused by a stroke can be effectively reduced by acute early intervention **NIHSS** Glascow Coma scale Cincinnati Stroke Scale ASSESSMENT OF sTROKE
STAT CT head without contrast/ PERFUSION? Stat Labs: CBC, BUN/Cr, lytes, aPTT/PT/INR, blood glucose Stat EKG NEURO AND NEUROENDOVASCULAR CONSULTS! NPO until Swallow Eval by speech therapy TTE/TEE/Echo Carotid Dopplers CXR Fasting lipid profile Work up
Superior to CT for small infarcts, especially in posterior or vertebrobasilar circulation CT Angiography Head/Neck also useful. MRI

![CP = E[ s 2 , s 5 , s 1 , s 3 , s 2 ’ , s 3 ’ , s 4 , s 1 ’ , s 4 ’ , s 5 ’ ] S[] I[]](https://cdn3.slideserve.com/6546826/slide1-dt.jpg)