New Oral Anticoagulation
190 likes | 772 Vues
New Oral Anticoagulation. Helen Livett Nurse Practitioner – Gastroenterology Alexandra Hospital Email: liveth@worcsacute.nhs.uk BSc Nursing Studies, awaiting completion of MSC in Advanced Practice

New Oral Anticoagulation
E N D
Presentation Transcript
New Oral Anticoagulation Helen Livett Nurse Practitioner – Gastroenterology Alexandra Hospital Email: liveth@worcsacute.nhs.uk BSc Nursing Studies, awaiting completion of MSC in Advanced Practice JAG Accredited Endoscopist – OGD, Flexible Sigmoidoscopy, Colonoscopy and some therapeutic endoscopic procedures Train the trainers JAG accreditation Non Medical Prescriber – Supplementary and Independent
Introduction • In 2011 new oral anticoagulants became available for the management of patients with atrial fibrillation and for the treatment and prevention of thromboembolic disease (deep vein thrombosis and pulmonary embolus). • These medications are becoming increasingly popular as they do not require blood monitoring in the same was as warfarin. • There is increasing evidence regarding the safety of these medications and recently guidelines on how patients on these medications should be managed for an endoscopic procedure have been published.
The purpose of this presentation is to: • Summarise the information available regarding these new medications, their pharmacology and the coagulation pathway. • Review the impact of these medications in preparing for and recovering from an endoscopy. • A checklist is presented which should enable nursing staff to facilitate the safety of patients on these medications undergoing an endoscopy.
Any patient undergoing elective surgery or endoscopy is at increased risk of bleeding when on anticoagulant or antiplatelet medications. The British Society of Gastroenterology (2008) guidance regarding management of anticoagulant and antiplatelet therapy prior to endoscopy have previously focused on warfarin and the antiplatelet drugs (aspirin and clopidogrel (Veitch A et al., 2008)).
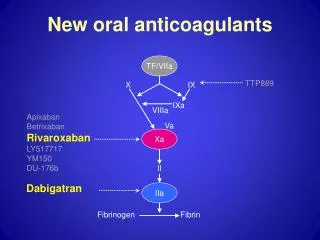
The onset of the new oral anticoagulants is rapid and predictable (Dolan G, 2012, Van Ryn J et al., 2013). • Anticoagulation is achieved after 2 – 3 hours or oral administration. The half-life for the new oral anticoagulants is short between 14 – 17 hours for Dabigatran and 4 – 9 hours for Ribaroxaban and excretion from the body is depending on renal clearance (Woodhouse C et al., 2013, BNF, 2013).
A major advantage of these new anticoagulants is that they do not require routine anticoagulant monitoring as warfarin does. In actual fact INR tests are unreliable in determining the effectiveness of agents (BNF, 2013) • For Dabigatran the APTT (activated partial thromboplastin time), diluted TT (thrombin time) and ecarin clotting time can be used to monitor the effectiveness of the drug(BNF, 2013). For Ribaroxaban, and apixoban the prothrombin time may provide a useful measure of the drug effect (Woodhouse C et al., 2013).
Side effects • The most common side effect is haemorrhage and patients should be monitored for signs of bleeding or anaemia; treatment should be stopped if severe bleeding occurs (BNF, 2013). In comparison to other anticoagulants the risk of bleeding with the new oral anticoagulants is equivalent with that observed for existing medications (Van Ryn J etal., 2013). • However other studies have reported the risk of life threatening bleeding were 1.8% higher in patients taking these new anti-coagulants compared to patients taking Warfarin (Connolly etal., 2010). There are no available antidotes (Campbell etal., 2011).
Haemorrhage should be managed supportively and with advice from a consultant haematologist. If the anticoagulation is stopped because of haemorrhage then the future requirement for anticoagulation should be discussed with a relevant specialist team, this may include haematology, cardiology, stroke specialists and gastroenterologists. • Other side effects are worth noting according to including dyspepsia, vomiting, a change in bowel habit, and deranged liver function tests (Woodhouse C et al., 2013).
Impact on Endoscopy • Woodhouse et al (2013) have reviewed the available literature regarding the practical management of patients taking these drugs and attending for endoscopic procedures and have suggested guidelines for the way in which these patients should be managed (Woodhouse C et al., 2013). They also suggest guidance as to the way in which haemorrhage secondary to endoscopy should be managed. The main concern is that there is no antidote and therefore coagulation is more difficult to achieve that it would be with a patient on warfarin (Woodhouse C et al., 2013) Therefore care must be taken to reduce the risks associated with these new agents(National patient safety agency, 2007) .
High risk and low risk procedures • Woodhouse C et al., 2013
Recommendations for Stopping Medications (Woodhouse et al, 2012)
Introduction of a Checklist • The Nursing and Midwifery Council (2008) state that nurses have a duty of care at all times (Nursing and Midwifery Council, 2008). They insist that nurses and healthcare professionals work with others to protect and promote the health and wellbeing of those in their care. • Responsibility and accountability for all • Protection for the nurses and the patients • Clear understanding and consistency of change to medication
Ronda et al. (2008) described the environmental conditions required to ensure safe medication practices (Ronda G et al., 2008). • These include: (a) the right to complete clearly written orders that specify the drug, dose, route, and frequency; (b) the right to have the correct drug route and dose dispensed from pharmacies; (c) the right to have access to drug information; (d) the right to have policies on safe medication administration; (e) the right to administer medications safely and to identify problems in the system; and (f) the right to stop, think, and be vigilant when administering medications (Ronda G et al., 2008).
A specific care pathway for this cohort of patients (see below) has been developed incorporating the guidance and evidence currently available (Woodhouse C et al., 2013). This should make pre-assessment as easy as possible. It will include a checklist for healthcare professionals to indicate and validate their decision making process. Patient information (verbal and written) on discharge from endoscopy regarding their continuation of oral anticoagulant drugs will also be clearly documented.
The protocol aims to minimise drug errors and place the onus of prescribing back with the referring consultant at the same time ensuring that communication with the patient and concordance is paramount guaranteeing that clarity of information is available.
References • BNF 2013. Oral anticoagulants In: BNF (ed.) British national formulary • CAMPBELL AR, MCKNIGHT R & HV, D. 2011. New anticoagulatns for thromboembolic disease implications. Journal of pharmacogenomics and pharmacoproteomics, 2, 104. • CONNOLLY S, EZEKOWITZ M, YUSUF S, EIKELBOOM J, OLDGREN J & PAREKH A 2010. Newly identified events in the RE-LY trial. Dabigatran versus warfarin in patients with atrial fibrillation. . NEJM, 363, 1139-1876. • CONNOLLY SJ, MD., E. & 2009. Dabigatran Versus Warfarin in Patients With Atrial Fibrillation. NEJM, 361, 1139-1151. • DOLAN G 2012. The evidence for dabigatranEtexilate in SPAF. Haematology news, 2. • GD, L. 2003. Virchow's triad revisited: abnormal flow. pathophysiolhaemostthromb, 33, 455-7. • GOODSTADT L & PONTING CP 2004. Vitamin K epoxide reductase: homology active site and catalytic mechanism. trends biochemsci, 29, 289-92. • GREEN J. Complications of Gastrointestinal endoscopy. British society of gastroenterology, 2006. • MANESH R, PATEL MD, MAHAFFEY KW & JYOTSNA GARG MS 2011. Rivaroxiban versus warfarin in non valvular atrial fibrillation. NEJM, 365, 883-891. • MUECK W, LENSING AWA, AGNELLI G & DECOUSUS H 2011. Rivaroxiban. population analyses in patients treated for acute deep vein thrombosis and exposure simulations in patients with atrial fibrillation treated for stroke prevention. Clinpharmacokinet, 50, 675-686. • NATIONAL PATIENT SAFETY AGENCY. 2007. Actions that can make anticoagulant therapy safer. NPSA patient safety alert 18 [Online]. http://www.nrls.npsa.nhs.uk/resources/. • NURSING AND MIDWIFERY COUNCIL. 2008. The code: standards of conduct, performance and ethics for nurses and midwives. [Online]. http://www.nmc-uk.org/nurses and midwives/standards and guidance1/the-code/the code in full/. • RONDA G, HUGHES & BLEGAN M 2008. Medication administration safety. . In: HUGHES R (ed.) Patient safety and quality: An evidence based handbook for nurses. Rockville • VAN RYN J, STANGIER J, HAERTTER S, LIESENFELD K & W, W. 2013. Dagigatranetexilate - a novel reversible, oral direct thrombin inhibitor: Interpretation of coagulation assays and reversal of anticoagulant activity International journal for vascular biology and medicine. , 103, 116-127. • VEITCH A, BAGLIN T, GERSHLICK A, HARNDEN S, TIGHE R & CAIRNS S 2008. Guidelines for the managament of anticoagulant and antiplatelet therapy in patients undergoing endoscopic procedures. Gut, 57, 1322-1329. • WOODHOUSE C, EVANS G & MULLER A 2013. The new oral anticoagulants: practical management for patietns attending for endoscopic procedures. BMJ; frontline gastroenterology 4, 213-218.