Download
1 / 33
480 likes | 2.06k Vues
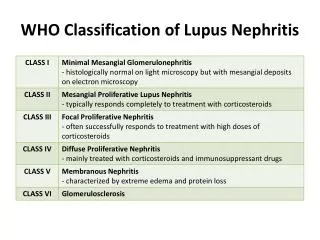
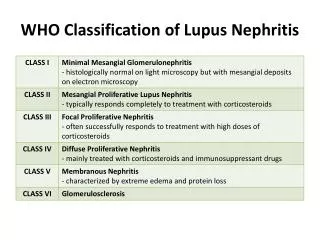
WHO Classification of Lupus Nephritis. International Society of Nephrology/Renal Pathology Society (INR/RPS) 2003 Classification of Lupus Nephritis. (LM – Light Microscopy, IF – Immunofluorescence Microscopy, EM – Electron Microscopy).

E N D
International Society of Nephrology/Renal Pathology Society (INR/RPS) 2003 Classification of Lupus Nephritis (LM – Light Microscopy, IF – Immunofluorescence Microscopy, EM – Electron Microscopy) Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
International Society of Nephrology/Renal Pathology Society (INR/RPS) 2003 Classification of Lupus Nephritis Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
International Society of Nephrology/Renal Pathology Society (INR/RPS) 2003 Classification of Lupus Nephritis (LM – Light Microscopy, IF – Immunofluorescence Microscopy, EM – Electron Microscopy) Weening et. al. 2004. The Classification of Glomerulonephritis in Systemic Lupus Erythematosus Revisited. J Am Soc Nephrol 15:241-250.
3. Enumerate the side-effects of cyclophosphamide • Side effects of Cyclophosphamide • diarrhea • lethargy • chemotherapy-induced nausea and vomiting • bone marrow suppression • darkening of the skin/nails • alopecia (hair loss) or thinning of hair • changes in color and texture of the hair • hemorrhagic cystitis Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
3. Enumerate the side-effects of cyclophosphamide • Side effects of Cyclophosphamide • carcinogenic, potentially causing transitional cell carcinoma of the bladder as a long-term complication • lower the body's immune system • cause temporary or (rarely) permanent sterility. Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
Some side effects with cyclophosphamide are potentially serious and should be reported immediately to a healthcare provider. These include but are not limited to: • Signs of an infection, such as chills or a fever • Blood in the stool • Blood in the urine (which can be a sign of bladder damage) • Severe mouth sores • Signs of an allergic reaction, including unexplained rash, hives, itching, and unexplained swelling. • Severe nausea, vomiting, or diarrhea • Decreased urination, which may be a sign of kidney damage • Difficulty breathing or water retention, which may be signs of congestive heart failure • Any unusual moles, skin sores that do not heal, or unusual lumps (which can be signs of new tumors or cancers) Reference: http://www.drugs.com/sfx/cyclophosphamide-side-effects.html
Clinical and radiographic manifestations of musculoskeletal TB
TB of Bones and Joints • Weight-bearing joints • spine 40% • hips 13% • knees 10%ff • Phemister’s Triad • Juxta-articular osteoporosis • Peripherally located osseous erosions • Gradual narrowing of the intra-osseous space Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of Internal Medicine, 17th Edition. McGraw-Hill. USA
Pott’s Disease (Tuberculous Spondylitis) • most dangerous form of musculoskeletal TB • bone destruction, deformity, and paraplegia • Progressive bone destruction, >2 adjacent vertebral bodies • leads to vertebral collapse and kyphosis(due to collapse in anterior spine) • Spinal canal narrowing: abscesses, granulation tissue or direct dural invasion • leading to SC compression and neurologic deficits Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of Internal Medicine, 17th Edition. McGraw-Hill. USA
Clinical Manifestations • Back pain, stiffness • thoracic and lumbosacral region most common • Constitutional symptoms = fever, weight loss • Most deadly complication = paraplegia • due to abscess compressing the spinal cord Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of Internal Medicine, 17th Edition. McGraw-Hill. USA
Radiographic Findings • Lytic destruction of anterior portion of vertebral body • Increased anterior wedging • Collapse of vertebral body Reference: Emedicine. 2009. Pott’s Disease. Retrieved February 16, 2010 from http://emedicine.medscape.com/article/226141-overview
CT Scan • provides better bony detail of irregular lytic lesions, sclerosis, disk collapse and disruption of bone circumference • reveals early lesions and is more effective for defining the shape and calcification of soft-tissue abscesses. Reference: Emedicine. 2009. Pott’s Disease. Retrieved February 16, 2010 from http://emedicine.medscape.com/article/226141-overview
Radiographic Manifestation CT scan demonstrating destruction of the right pedicle of T10 due to Pott's disease Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of Internal Medicine, 17th Edition. McGraw-Hill. USA
Tuberculosis of Hip and Knee Joints • Unrecognized joint destruction • Hip joints • Involves the head of the femur (common) • Painful • Knee joints • Pain and swelling • Diagnosis: biopsy, tissue culture and synovial fluid exam (thick in appearance, high protein concentration and variable cell count) Reference: Fauci. Braunwald. Kasper. Hauser. Longo. Jameson. Loscalzo. 2008. Harrison’s Principles of Internal Medicine, 17th Edition. McGraw-Hill. USA
Tuberculosis of the Hip Lesion on femoral head and acetabulum Kissing Lesion: hallmark of TB infection Reference: Singh, Arun Pal. 2009. X-Ray of TB of Hip Joint. Retrieved February 16, 2010 from http://boneandspine.com/muculoskeletal-radiology/xray-of-tuberculosis-of-hip-joint/
calcified debris in the supra-patellar bursa Reference: Palmer & Reeder. 2009. The Imaging of Tropical Diseases. Retrieved February 16, 2010 from http://www.isradiology.org/tropical_deseases/tmcr/chapter5/lymphadenopathy.htm
Clinical, laboratory, radiographic manifestations of genitourinary TB
Clinical Manifestations • Local symptoms predominate • Up to one third of patients may concomitantly have pulmonary manifestations • Common symptoms include: • Urinary frequency • Dysuria • Nocturia • Hematuria • Abdominal and Flank pain Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
Clinical Manifestations • In females: • May affect the fallopian tubes and the endometrium causing infertility, pelvic pain and menstrual abnormalities • In males: • Primarily affects the epididymis, producing a slight tender mass that may drain externally through a fistulous tract; orchitis and prostatitis. Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
Laboratory Manifestations • Urinalysis: • Pyuria and Hematuria • Urine Culture: • Pyuria but negative for common organisms causing UTI • Culture of three morning urine specimens positive for Mycobacterium tuberculosis is a definitive diagnosis. Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
Radiographic Manifestations • Intravenous pyelography • Abdominal CT • MRI Deformities, obstructions, calcifications and ureteral strictures are suggestive findings in genitourinary tuberculosis. Harrison’s Principle of Internal Medicine, 17th ed. P1011-1012
Isoniazid • Isoniazid-induced hepatitis-most common major toxic effect • Peripheral neuropathy • CNS toxicity-memory loss, psychosis,seizures • Fever and skin rashes • Drug-induced SLE • Hematologic abnormalities • Provocation of pyridoxine deficiency anemia • Tinnitus • Gastrointestinal discomfort Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 773
Rifampicin • Orange urine, sweat and tears • Rashes • Thrombocytopenia • Nephritis • Light-chain proteinuria • Flu-like sydrome(fever, chills, myalgia, anemia and thrombocytopenia) Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 774
Ethambutol • Retrobulbar neuritis • most common serious adverse event • Loss of visual acuity and red-green color blindness • Hypersensitivity syndrome consisting of cutaneous reaction (such as rash or exfoliative dermatitis) • Fever and lymphadenopathy Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 774 http://www.drugs.com/sfx/ethambutol-side-effects.html
Pyrazinamide • Hepatotoxicity-major adverse effect • Nausea • Vomiting • Fever • hyperuricemia Katzung, B, Basic and Clinical Pharmacology 10th ed., McGraw Hill 2007, page 775
Anti-TB regimen in special situations of liver disease, renal impairment, and pregnancy.
Liver disease • Patients with pre-existing liver disease can receive the usual TB regimens provided that there is no clinical evidence of chronic liver disease, hepatitis virus carriage, a past history of acute hepatitis, current excessive alcohol consumption. • However, hepatotoxic reactions to anti-TB drugs may be more common among these patients and should therefore be anticipated • The first-line drugs HRZ are all associated with hepatotoxicity. • Pyrazinamide is the most hepatotoxic Treatment of tuberculosis: guidelines - 4th ed. WHO http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf
If the serum AST level is more than 3 times normal before the initiation of treatment, the following regimens should be considered . • Two hepatotoxic drugs (rather than the three in the standard regimen): 9 months of HRE 2 months of HRSEfollowed by 6 months of HR 6–9 months of RZE. • One hepatotoxic drug: 2 months of HES, followed by 10 months of HE • No hepatotoxic drugs: 18–24 months of streptomycin, ethambutol and a fluoroquinolone. • The more unstable or severe the liver disease is, the fewer hepatotoxic drugs should be used. • In general, patients with chronic liver disease should not receive pyrazinamide. All other drugs can be used, but close monitoring of liver enzymes is advised.
Renal impairment • The recommended initial TB treatment regimen for patients with renal failure or severe renal insufficiency is 2 months of HRZE, followed by 4 months of HR. • Isoniazid and rifampicin are eliminated by biliary excretion, so no change in dosing is necessary. • There is significant renal excretion of ethambutol and metabolites of pyrazinamide and doses should therefore be adjusted. • Three times per week administration of these two drugs at the following doses is recommended: pyrazinamide (25 mg/kg), and ethambutol (15 mg/kg) Treatment of tuberculosis: guidelines - 4th ed. WHO http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf
Renal impairment • While receiving isoniazid, patients with severe renal insufficiency or failure should also be given pyridoxine in order to prevent peripheral neuropathy. • Streptomycin should be avoided in patients with renal failure because of an increased risk of nephrotoxicity and ototoxicity. • If streptomycin must be used, the dosage is 15 mg/kg, two or three times per week, to a maximum of 1 gram per dose, and serum levels of the drug should be monitored.
Pregnancy • Women of childbearing age should be asked about current or planned pregnancy before starting TB treatment. • A pregnant woman should be advised that successful treatment of TB with the standard regimen is important for successful outcome of pregnancy. • With the exception of streptomycin, the first line anti-TB drugs are safe for use in pregnancy • streptomycin is ototoxic to the fetus and should not be used during pregnancy. • Pyridoxine supplementation is recommended for all pregnant women taking isoniazid Treatment of tuberculosis: guidelines - 4th ed. WHO http://whqlibdoc.who.int/publications/2010/9789241547833_eng.pdf