Lupus Nephritis
Lupus Nephritis. Introduction. 60 – 75% of pts with SLE Probably the most serious complication Differs in clinical pattern, severity , prognosis & treatment. Pathogenesis. Autoimmune. MHC II on APC/ B cell. Costimulatory molecules Eg. CD 40/ 40L B7/ CD 28 B7/ CTLA4. T cell.

Lupus Nephritis
E N D
Presentation Transcript
Introduction • 60 – 75% of pts with SLE • Probably the most serious complication • Differs in clinical pattern, severity , prognosis & treatment
Pathogenesis • Autoimmune MHC II on APC/ B cell Costimulatory molecules Eg. CD 40/ 40L B7/ CD 28 B7/ CTLA4 T cell Polyclonal B cell activation Formation of autoreactive antibodies vs nuclear Ag & other self Ag Ab/ Ag complexes ( preformed or in situ) Binding & damage to GBM C’ activation Recruitment of polys & mononuclear cells RENAL DAMAGE
GLOMERULUS Mesangial deposits Subendothelial & mesangial Subepithelial Widespread scarring Interstitium Tubules Vessels Histologic class II III & IV V VI Pathology
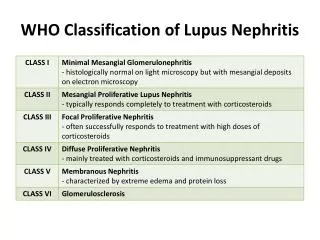
WHO Classification of LN • I. Normal glomeruli • Normal by all techniques • Normal on LM but deposits on immunohistology & / or EM • II. Pure mesangial alterations • A. mesangial widening & /or mild hypercellularity • B. mesangial cell proliferation • III. Focal segmental GN ( focal proliferative GN) • A. active necrotising lesions • B. active sclerosing lesions • C. sclerosing lesions
WHO Classification of LN ( cont.) • IV. Diffuse proliferative GN • ( severe mesangial/ mesangiocapillary with extensive subendothelial deposits. Mesangial deposits always present & frequent subepithelial deposits) • A. with segmental lesions • B. With active necrotising lesions • C. with active & sclerosing lesions • D. with sclerosing lesions • V. Diffuse membranous GN • A. Pure membranous GN • B. associated with lesions of category II • VI. Advances sclerosing GN
Renal manifestations • Tend to appear within the 1st 2yrs of SLE • Almost ½ have asymptomatic urine abnormalities • Proteinuria - dominant feature • Haematuria – almost always present but not in isolation • Nephrotic • Severe nephritis • ARF occassionally • GFR in ½ • Revised criteria for classification of SLE • Proteinuria >0,5g / day or 3+ • Casts – rbc/ granular/ tubular/ mixed
Lab investigations • Monitoring with regular urinalysis & serum creatinine • Screen all pts with proteinuria for ANA • Anti ds DNA • In about 60% with SLE • Levels often reflect disease activity • with Rx ( ANA remains +) • If normal – safe to Rx in chronic phase • complement • In ¾ untreated esp. with nephritis • APLA In 1/3 to ½ Associated with renal arterial, venous & glomerular thrombosis
Clinicopathologic correlates • Many are asymptomatic & insidiously progressive • More severe histologic forms tend to have more severe clinical findings • But histology cannot be predicted with certainty • No clinical features - may have significant glomerular disease on biopsy BIOPSY NB
Indications for renal biopsy • Clinical + lab features = DPGN • Biopsy may not be necessary prior to Rx • Abnormal clinical + lab features • Lowgrade • Compatible with more than one form of LN • Biopsy may alter Rx
Histology • 1995 WHO Classification of Lupus Nephritis • > ½ Class III – IV • 10 – 15% class V • Focus on glomerular lesions • 50% of changes in interstitium • In a few ATN occurs in absence of glomerular disease ARF • Glomerular lesions not static • May undergo transition with time eg from Class IV to V with Rx
NIH activity – Chronicity index • 2nd classification • Assessment of inflammation ( activity) & permanent damage from scarring & fibrosis (chronicity) • Includes glomeruli & TIN features • Useful for prognosis, guide to Rx • > Chronicity = worse outcome • Helpful to monitor Rx response on repeat biopsies
Prognosis • Predictors of poor prognosis: • Black race • Male • Anaemia • creatinine • Nephrotic range proteinuria • Glomerular & tubulointerstitial scarring • Severe tubulointerstitial nephritis • Chroniciy index > 3
Treatment aims • Recognise early renal involvement • Induce & maintain remission & decrease risk of progression to ESRD • Minimise Rx related toxicity ( esp. during maintenance phase )
Treatment • Induction • Maintenance • short courses associated with relapses
Treatment options (1) • Corticosteroids (CS) • In all groups • No trials of CS vs no CS • Pulse medrol – no formal studies; impression of rapid control • Cyclophosphamide ( CP) • Intermittent pulse CP = DOC in mod – severe disease • Oral CP – used < 2-3/12 ( S/E s) • Infections, cervical dysplasia, gonadal toxicity • Azathiaprine (Aza) • Remarkably safe • Leucopaenia, hepatotoxicity, marginal risk of malignancy • Safe in pregnancy • Primary Rx in mild forms & in pts strongly oppposed to CP
Treatment options (2) • Mycophenolate mofetil (MMF) • Toxicity of CP prompted a search for effective less toxic Rx for LN • Inhibits de novo pathway of purine synthesis lymphocyte production • Leukopaenia, nausea, diarrhoea, infections • Shown to be effective but concern re relapse in severe disease • Recent trial : ‘short term Rx with IVI CP followed by maintenance Rx with MMF or Aza …more efficacious & safer than long-term Rx with IVI CP.’ • ( NEJM march 4, 2004 vol 350 (10) 971- 80)
Treatment options (3) • Cyclosporin A • Evaluated in extrarenal manifestations ; few studies in LN • Corticosteroid sparing effect in children • flares of disease activity during Rx or when the drug is tapered • may be used in combination with other immunosuppressives • should not be used as monotherapy • Low dose – no permanent nephrotoxicity • Monitor levels if higher doses used • Monitor renal function • Plasmapharesis • no benefit
Mild mesangial LN • good prognosis • no specific therapy • more aggressive disease • oral CS • AZA if initial response is poor
Proliferative GN (1) • Immunosuppression most beneficial • NIH Rx trials : • CS alone and CS +AZA / oral CP/ AZA + CP/ monthly IV CP. • CP better than CS alone • IV CP + low dose prednisone better than high dose prednisone alone • AZA had an intermediate response, but no significant difference between AZA & CS
Proliferative GN (2) • Intial high dose CS (prednisone 1mg/kg/day) + pulse IV CP (750-1000 mg/m2 BSA). • pulse of CP is given at monthly interval x 6/12 • then every 3/12 x two years. • CS gradually tapered • Alternative to high dose oral steroids • Pulse IV methylprednisolone, + low dose oral prednisone (10-20 mg/day) to the incidence of steroid side-effects • Initial IV methylprednisolone, 12 weeks oral CP ( 1-3 mg/kg/day) followed by combined AZA and CS
Proliferative GN (3) • Euro-Lupus regimen. • Induction: limited course of low dose IV CP (6 fortnightly pulses of 500 mg) • followed by a safer cytotoxic drug, AZA, as a long-term maintenance Rx • Data from the Euro-Lupus Nephritis Trial (ELNT) suggest that such a low cumulative dose of CP may achieve good clinical results, though important differences in patient populations between the ELNT and NIH studies, as well as in the dosing of CP, preclude extrapolation to other LN populations with different ethnic backgrounds or disease severity
Membranous GN • progression to ESRD • 20 % in 10 yrs • Membranous GN with non nephrotic proteinuria • No Rx • Monitor progression
Membranous GN • Limited data on Rx • Rx follows that of idiopathic membranous nephritis • Steroids should not be used as sole therapy • AZA is not associated with any significant benefits • Alkylating agents, CP and chlorambucil - both effective • for patients with clinical features that predict a high likelihood of progression to ESRD, such as severe or prolonged nephrosis, renal insufficiency or HT • Cyclosporin • -if alkylating agents are contraindicated or ineffective • Limited experience suggests that most will experience a reduction in proteinuria. • Early results from an NIH study of membranous LN • prednisone alone vs prednisone + CyA or CP • more favourable response to CP • frequency of relapse with CyA treatment may be significant
Newer forms of Rx • High dose immunoablative Rx • For refractory cases • CP, antithymocyte globulin & methylprednisolone haematopoietic stem cell transplantation • Long-term follow-up of reported cases & randomized trials necessary • Biological approaches • Anti-CD40L and CTLA4Ig. • Results of murine studies are encouraging
Chronic renal failure • Nonimmune mechanisms • BP control • Low protein diet • Low salt • Calcium & vitamin D • EPO • nephrotoxic drugs
Prognosis • > 30 yrs ago • few pts with severe class IV nephritis survived > 1-2 yrs • ½ with less severe disease died within 5 yrs • Marked improvement in Rx • 10 – 15% progress to ESRF • Sepsis = major cause of death • Transplant • recurrence rare