Download
1 / 1
10 likes | 225 Vues
Low HCV Treatment Rates after a Liver Biopsy O.M Adeyemi , B. Attar, G. Huhn , D. Wolen , M. Gallagher, R. Goldberg CORE Center, Stroger Hosp. of Cook County, Chicago, IL and Rush Medical College,Chicago , IL. 48 th ICAAC/IDSA meeting, Washington, DC October 25-28, 2008. V-1637.

E N D
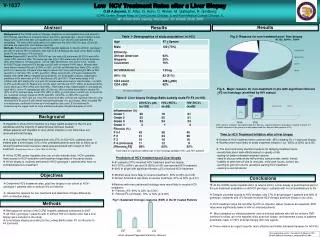
Low HCV Treatment Rates after a Liver Biopsy O.M Adeyemi, B. Attar, G. Huhn, D. Wolen, M. Gallagher, R. Goldberg CORE Center, Stroger Hosp. of Cook County, Chicago, IL and Rush Medical College,Chicago, IL. 48th ICAAC/IDSA meeting, Washington, DC October 25-28, 2008 V-1637 Predictors of HCV treatment post Liver biopsy Abstract Results Results Background-At the CORE center in Chicago, despite an on-site hepatitis clinic and access to HCV therapy regardless of insurance status, few HCV+ genotype (gn) 1 pts are treated. A liver biopsy (LB) is performed after >2 hepatitis clinic visits in gn1 pts who are treatment (Rx) candidates. The aims of this study were (1) to determine the rate of HCV Rx post LB and (2) delineate the reasons for non-treatment post LB. Methods- Retrospective review of the CORE hepatitis database to identify all HCV+ genotype 1 pts (with or without HIV co-infection), who had a LB. LB Staging was done using Batts-Ludwig scale: F0 (no fibrosis) to F4 (cirrhosis). Results-Between 8/01 and 8/06, 163 HCV+gn1 pts had a LB performed; 83 (51%) were HIV+ (mean CD4, cells/mm 428). The mean age was 47yrs; 75% were male, 63% African American (AA), 20% Hispanic, 16%Caucasian. On LB, 58% had Fibrosis >F2 and 11% F4. Overall, 61/163 [37%] pts received HCV therapy post LB; with no impact of HIV status. Women were more likely to receive Rx post LB (50% vs 32%, p=0.05) and AA were less likely (27% vs 50% p=0.01) to receive Rx. Pts were more likely to receive Rx if they had; fibrosis>F2 48% vs 22% (p=0.001) or cirrhosis 70% vs 34% (p=0.001). When only pts with >F2 were considered Rx eligible, then 46/93 [49%] of eligible pts received Rx. On multivariate analysis, independent predictors of Rx were race (p=0.01) and fibrosis >F2 (p=0.001). There were delays in Rx initiation with 45% starting Rx >1yr post LB; women were more likely to start Rx later, >1yr (65% vs 35% p=0.05) post LB. Reasons for non-Rx were; mild fibrosis F0-F1 (53%), pt declined (20%), lost to follow up (LTFU) (19%) and other (8%). There were 2 liver related deaths in untreated pts (both HIV+). In the 47 untreated pts with >F2 fibrosis, HIV+ pts were more likely to decline Rx (57% vs 27%) and less likely to be LTFU (23% vs 59%) (p=0.04) when c/w HIV- pts. In the 61 Rx pts, sustained virologic response (SVR) was 26% (14%HIV+ vs 38% HIV-) (p=0.04). Conclusions; In HCV+ gn1 pts, only 37% overall and 49% of those with significant fibrosis (>F2) received HCV Rx post LB with almost half starting therapy >1yr post biopsy. Most untreated HIV co-infected pts, continued to follow up in the hepatitis clinic post LB, but declined Rx underscoring the urgent need for more effective and better tolerated therapies for HCV. Table 1- Demographics of study population ( n=163) Fig 2- Reasons for non treatment post- liver biopsy N=102; 52HIV+, 50HIV- Fig 3- Major reasons for non-treatment in pts with significant fibrosis >F2 on histology (stratified by HIV status) All values mean+2SD P=0.04 Table 2- Liver biopsy findings Batts-Ludwig scale F0-F4 (n=163) Background (N=28) (N=22) • -Hepatitis C Virus (HCV) infection is a major health problem in the US and worldwide and the majority of patients have not been treated. • Most patients with Hepatitis C virus (HCV) infection in our clinic have not received antiviral therapy. • -A study from New York showed that only 37% of 433 HCV+ patients were treated after a liver biopsy. 53% of the untreated patients were lost to follow up or refused treatment and insurance status was associated with receipt of HCV treatment. (Narasimhan G et al, J. Virol 2006:13;783-786). • -At the CORE center hepatitis clinic (an on-site referral clinic), HCV+ patients have access to HCV evaluation and treatment regardless of insurance status. • -A liver biopsy is routinely performed in HCV genotype 1 patients who have no contraindications to treatment. Other reasons included-: decompensated liver disease, ongoing alcohol or drug abuse, medical or psych C/I 2 deaths occurred in this group from decompensated liver disease (both patients HIV+) Time to HCV Treatment Initiation after a liver biopsy • -Delays in HCV treatment were common with 45% initiating Rx >1 year post biopsy. • -Women were more likely to delay treatment initiation >1yr (65% vs 35%) (p=0.05). • -The most commonly identified reasons for delaying treatment were; • -anxiety/fear about side effects/impact on quality of life. • -waiting for better tolerated treatment options. • -need to discuss extensively with primary care provider, family, friends • -Inability to take time off due to new jobs, child-care issues, school, etc. • -wanting to get CD4 counts up before starting HCV treatment • -seeking a second opinion There were no significant differences in liver histology between HIV+ and HIV- patients • -61 patients (37%) received HCV treatment post liver biopsy. • 31 (37%) of HIV+ pts and 30 (38%) of HIV- pts received HCV treatment. • -49% of all pts with significant fibrosis (>F2) received HCV treatment • -Women were more likely to receive treatment- 50% vs 32% (p=0.05) • -African Americans less likely to receive treatment- 27% vs 50% (p=0.01) • Patients with more advanced histology were more likely to receive HCV treatment; • - Fibrosis >F2- 49% vs 22% (p=0.001) • - Fibrosis F4-(cirrhosis)- 70% vs 34% (p=0.001) Objectives Conclusions • -Determine HCV treatment rates, post liver biopsy in our cohort of HCV+ genotype 1 patients with or without HIV co-infection. • - Assess the reasons for non-treatment and determine if these differed by HIV co-infection status. • -At the CORE center hepatitis clinic (a referral clinic), a liver biopsy is performed as part of the pre-treatment evaluation on all HCV genotype 1 patients with no contraindications to Rx • -Despite universal access to HCV therapy; only 37% of all genotype 1 patients and 49% of genotype 1 patients with >F2 fibrosis received HCV therapy post liver biopsy in our clinic. • -HCV treatment rates did not differ by HIV co-infection status, however as expected, SVR rates were significantly lower in HIV co-infected patients. • - Most untreated co-infected patients and co-infected patients who did not achieve SVR continue to follow up in the hepatitis clinic post liver biopsy and represent a pool of patients potentially ready for HCV antiviral therapy with new agents. • -There remains an urgent need for more effective and better tolerated therapies for HCV Rx. Fig 1; Sustained Virologic response (SVR) in the 61 treated Patients Methods • -Retrospective review of the CORE hepatitis database conducted in 2007. • -All HCV+ genotype 1 patients with or without HIV co-infection who had a liver biopsy were included in the study. • -Liver biopsy staging according to the Ludwig-Bartts scale; F0 (no fibrosis) to F4 (cirrhosis) N=61 N=31 N=30 Corresponding author: Oluwatoyin M Adeyemi, MD Email address: oluwatoyin_adeyemi@rush.edu All pts received Pegylated Interferon+ Ribavirin