Download
1 / 50
640 likes | 2.48k Vues
Common Injections for the Family Physician : General Principles. Francis G. O’Connor, MD, MPH Department of Military and Emergency Medicine Medical Director, Consortium for Health and Military Performance Uniformed Services University of the Health Sciences. Objectives.

E N D
Common Injections for the Family Physician :General Principles Francis G. O’Connor, MD, MPH Department of Military and Emergency Medicine Medical Director, Consortium for Health and Military Performance Uniformed Services University of the Health Sciences
Objectives • Review the indications, benefits, risks, and contraindications of injections in Family Medicine. • Describe general principles involved in administering injections to include consent, equipment, anesthesia, choice of corticosteroid and technique. • Discuss basics of coding for the procedure.
Diagnosis: synovial fluid analysis therapeutic trial imaging studies synovial biopsy Therapy: remove tense effusions remove blood or pus injection of steroids or other intra-articular therapies therapeutic lavage Indications
Benefits - Cochrane Reviews • Intraarticular corticosteroid for treatment of osteoarthritis of the knee • The short-term benefit of IA corticosteroids in treatment of knee OA is well established, and few side effects have been reported. Longer term benefits have not been confirmed based on the RevMan analysis. The response to HA products appears more durable. • Corticosteroid injections for shoulder pain • Despite many RCTs of corticosteroid injections for shoulder pain, their small sample sizes, variable methodological quality and heterogeneity means that there is little overall evidence to guide treatment.
Risks/Complications • Infection: one infection per 20,000 to 50,000 injections. • Tendon rupture • Post-injection flare • Atrophy/hypo-hyperpigmentation • Cartilage degeneration • Hyperglycemia • Local trauma
Contraindications • Cellulitis or broken skin over needle entry site • Anticoagulation or a coagulopathy • Intra-articular fractures • Septic effusion • Lack of response to prior injections • More than three prior injections in the last year to a weight bearing joint. • Inaccessible joints; joint prostheses.
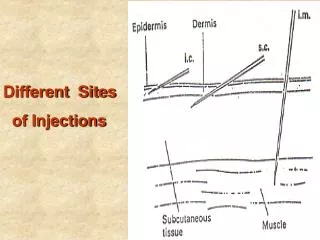
General Principles • Consent • Equipment • Anesthesia • Corticosteroids • Technique • Post-Procedure Care
Consent • Consent should be obtained on all diagnostic and therapeutic injections! • A detailed discussion of benefits, risks and the expected results should be covered. • Consent should be witnessed and documented.
Equipment • Controversies: • sterile prep vs. alcohol prep • sterile gloves vs. nonsterile • 21 to 27 gauge needles for injections; 18 to 20 gauge for aspirations • 1 to 10cc syringes for injections; 3 to 50cc for aspirations • ethyl chloride, 1 and 2% lidocaine, 0.5% bupivicaine • sponges, Band-Aids • access to equipment for allergy/anaphylaxis
Anesthesia • Aids in providing pain relief, assisting in diagnosis, and providing a volume for the steroid. • Lidocaine: 0.5% to 2%; amide; 1 to 2 min onset of action; duration 1 hr. • Bupivicaine: 0.25 to 0.5%; amide; 30 minute onset of action; duration 8 hr. • Single versus multi-dose vials • Ethyl chloride
Anesthesia • Anesthetics work by causing a reversible block to impulse conduction along nerve fibers. Loss of Pain Sensation Loss of All Sensation Loss of Motor Power As Dose of Local Anesthetic Increases
Corticosteroids • Mechanism of Action: complex and largely unknown, however, they do: • Reduce cytokines and inflammatory mediators; • Decrease capillary permeability; • Decline in PMN migration. • Treats the local inflammatory response, not the clinical problem. • Maximize glucocorticoid effects; minimize mineralocorticoid effects. • Increased solubility = shorter duration = lower risk for post-injection steroid flare = lower risk for local atrophy.
Hylauronic Acid Derivatives • FDA classifies these agents as devices, not drugs. • Indicated only for treatment of knee osteoaarthritis. • Hylan G-F20 polymers: • Heavy weight preparations • Synvisc • Three weekly injections • Sodium Hyaluronate • Hyalgan • Five weekly injections
Hyalgan • Synovial fluid is an ultrafiltrate of plasma modified by the addition of hyaluronic acid (HA), which is produced by the synovium. • In osteoarthritis, the HA is decreased and compromised. • Exogenous supplementation of intraarticular HA is thought to support changes in the character of synovial fluid.
Mixing Agents • First, draw the anesthetic into the syringe; • Second draw the corticosteroid into the syringe; • Next draw 1cc of air into the syringe to create a “mixing bubble”; • Prior to injection, mix the agents, and then expel the air prior to injection.
Technique • Patient • Be prepared! • Landmarks • Aseptic vs. Sterile technique • Local anesthesia • Needle insertion • Delivering the volume: • bolus vs. peppering
Ultrasound Guidance • Ultrasound guidance is an accurate method for the delivery of therapeutic injections in the musculoskeletal system. • The visualization of the needle in real time allows for reliable placement of the needle tip in the tendon sheath, bursa, or joint of interest. • Both superficial and deep articulations and tendon sheaths can be targeted for diagnostic or therapeutic interventions. • In addition, intratendinous calcifications, the plantar fascia, and interdigital (Morton's) neuromas can also be visualized and injected directly under real-time guidance. • Performing percutaneous interventions with ultrasound ensures accurate needle tip placement and helps direct the needle away from other regional soft-tissue structures such as nearby neurovascular bundles.
Trigger Point Injections • A 22-gauge, 1.5-inch needle is usually adequate to reach most superficial muscles. • Using sterile technique, the needle is then inserted 1 to 2 cm away from the trigger point so that the needle may be advanced into the trigger point at an acute angle of 30 degrees to the skin. • A small amount (0.2 mL) of anesthetic should be injected inside the trigger point. The needle is then withdrawn to the level of the subcutaneous tissue, then redirected superiorly, inferiorly, laterally and medially, repeating the needling and injection process in each direction until the local twitch response is no longer elicited or resisting muscle tautness is no longer perceived.
Post-Procedure Care • Evaluation of patient relief in the office • Discussion of steroid effects/expectations • Afterpain treatment • Ice vs. short course NSAID • Activity Recommendations • Rest weight bearing joints for several days to a week. • Follow-up visit!
Post-Injection Flare vs. Infection • Post-Injection Flare: • Reaction caused by development of steroid crystals in the synovial space; may also be the result of chemical synovitis from methylparaben in multi-dose anesthetic vials. • Occurs 6 to 24 hrs s/p injection; may last 2 to 4 days. • Consider aspiration to r/o infection. • Infection: • Uncommon. • Symptoms persist over 72 hrs. • Warmth, redness, streaking, fever. • Confirmed by aspiration.
Pain Relief and Injection Therapy Corticosteroid Anesthetic Pain Threshold 48hrs Time
Injection Frequency • No EBM guidelines. • General Recommendations: • Limit injections to large joints to 4 times per year; no more than 10 times overall. • Small joints should be injected no more than three times per year and four times overall. • Steroid injections should be spaced at least 4 weeks apart; hyaluronan injections 6 months apart.
Coding • Reimbursement requires clinicians properly identify two, possibly three, appropriate codes: • The Diagnosis: • International Classification of Diseases, 9th Revision ICD-9 • The Procedure: • Current Procedural Terminology CPT • The Drug Utilized: • “J” Code • Evaluation and Management (E/M) Codes are dependent upon New patient status.
Coding – “J” Codes “J” Codes for Injectable Corticosteroids
Subacromial Space • Indications: • relief of pain in subacromial impingement syndrome • diagnostic to help r/o adhesive capsulitis or rotator cuff tear, or confirm RTC impingement
Subacromial Space • Clinical anatomy landmarks: • AC joint • posterolateral recess between the humeral head and the acromion
Subacromial Space • Technique • seated patient • arm relaxed with other arm used for passive traction • ethyl chloride or 1% lidocaine anesthesia • inferior to posterolateral acromion • needle bevel up oriented cephalad and directed toward the anterior acromion • bolus insertion
Subacromial Space • Needle size and dosage: • 1 ml of corticosteroid (celestone soluspan or kenalog) with 50/50 mix of 6 to 9 ml of lidocaine and marcaine in a 10ml syringe. • 18 gauge needles for medicine draw; 22 gauge 11/2 needle for injection
Lateral Tennis Elbow • Indications: • lateral tennis elbow that fails to improve with conservative therapy
Lateral Tennis Elbow • Clinical anatomy/landmarks • radial head, appreciated by pronation/supination • humeral lateral epicondyle • extensor carpi radialis brevis
Lateral Tennis Elbow • Technique: • supine or seated • elbow in 90 degrees of flexion and supinated • area of maximal tenderness found; usually 1fingerbreadth distal and medial to the lateral epicondyle • needle inserted into a triangular fatty recess near the common extensor origin
Lateral Tennis Elbow • Needle size and dosage: • 25 to 27 gauge 1 inch needle • .5ml of celestone with 1ml of 1 or 2% lidocaine
Trochanteric Bursitis • Indications: • recalcitrant trochanteric bursitis
Trochanteric Bursitis • Clinical anatomy landmarks • greater trochanteric prominence • illiac crest • sciatic nerve
Trochanteric Bursitis • Technique: • patient in the lateral decubitus position • point of maximal tenderness identified • needle perpendicular to the skin • depth of insertion 1/2 to 3 inches • gentle “peppering” of the bursa
Trochanteric Bursitis • Needle size and dosage: • 22 to 25 gauge 11/2 inch needle • 1ml of celestone with 3 to 5ml of 1% lidocaine
Knee Joint • Indications: • inflammatory or degenerative arthritis • Remove tense effusion • diagnostic
Knee Joint • Clinical anatomy/landmarks • patellar tendon • inferior patellar pole • medial joint line • lateral joint line
Knee Joint • Technique: • seated or supine position with knee flexed to 90% • recess lateral and inferior to the patellar tendon border identified at the level of the joint line • needle directed toward the center of the knee • depth of insertion is >1.5” • GO DEEP
Knee Joint • Needle size and dosage: • 22 to 25 gauge 1-1/2+ inch needle • 10-40mg triamcinolone, +/- lidocaine
Myofascial Trigger Points • Indications: • diagnosis and treatment of myofascial trigger points
Myofascial Trigger Points • Clinical anatomy landmarks • dependent on location of trigger and tender points
Myofascial Trigger Points • Technique: • palpable as fusiform firm nodules • nodule trapped between the fingers of the nondominant hand • sterile prep • local “twitch” response • two to five sessions may be required
Myofascial Trigger Points • Needle size and dosage: • 25 to 27 gauge 1 inch needle • 1 to 5ml of 1 or 2% lidocaine
Conclusion • Injections, when done properly and with the right indications, are a tremendous asset to the practice of the family physician.