Download
1 / 50
660 likes | 1.68k Vues
Epidemiology and Pathophysiology of Intracerebral Hemorrhage. Edward C. Jauch, MD MS FACEP. 1.

E N D
Epidemiology and Pathophysiology of Intracerebral Hemorrhage Edward C. Jauch, MD MS FACEP 1
Edward C. Jauch, MD MS FACEPAssistant ProfessorAssociate Director of ResearchDepartment of Emergency MedicineUniversity of Cincinnati College of MedicineFaculty, Greater Cincinnati / Northern Kentucky Stroke Team 2
Global Objectives • Review epidemiology of ICH • Understand pathophysiology of ICH • Discuss lessons from acute ischemic stroke • Improve Emergency Medicine practice
Patient Initial Clinical History • 57 yo male with sudden onset headache and left sided weakness • Family calls 911 • EMS transport to OLFH Hospital • Enroute patients symptoms progress to full hemiplegia • Initial VS: 210 / 120 mmHg, HR 110, R 24
Patient ED Presentation • PMHX: HTN for 10 years, hyperlipidemia • SHX: Smoking 30 years • Meds: ACE inhibitor, ASA • ROS: No recent illness or injuries, no new medications
Patient ED Presentation • Physical examination: • VS - 220 / 140 mmHg, HR 110, RR 22, T 98.6oC • Uncomfortable WM, arouses to voice • HEENT/CV/Lungs/Abd - WNL • Neuro – • LOC mildly depressed • CN with L facial droop and partial gaze palsy, VFI • Motor with dense L hemiplegia • Sensory with mild L sensory loss • Speech slurred but no significant aphasia • NIHSS = 12
Key Questions • What is your differential diagnosis? • What are the most common ICH etiologies? • What is the pathophysiology of ICH? • What guidelines exist that govern the acute care of ICH patients? • What can be learned regarding ICH management from acute ischemic stroke? • How can the emergent care of ICH patients be enhanced?
Patient ED Presentation • Initial noncontrast CT scan • Labs: • CBC, chem 7 – WNL • PT, PTT – WNL • ECG – LVH with strain
Lacunar 19% Thromboembolic 6% SAH 13% Cardioembolic 14% Hemorrhagic 26% Ischemic 71% ICH 13% Unknown 32% Other 3% Stroke Subtypes Up to 65,000 ICH per year in U.S. (NINCDS Stroke Data Bank: Foulkes, Stroke, 1988)
ICH Classifications • Primary • Hypertensive arteriopathies • Cerebral amyloid angiopathies • Secondary • Neoplasms • Structural lesions • Anticoagulants or thrombolytic agents • Drugs (cocaine, ephedra, etc) • Traumatic brain injury
Location • Lobar • Associated with amyloid angiopathy • Nonlobar • Associated with hypertension • Cerebellar • Intraventricular
Lobar Hemorrhage • Secondary to cerebral amyloid angiopathy • Beta-amyloid deposition in vessels of cortex and leptomeninges • Associated with aging • Lobar hemorrhage in young due to AVM, cavernous hemangioma
Non-lobar Hemorrhage • Non-lobar or hypertensive hemorrhage • Associated with hypertensive arteriolosclerosis • Location • putamen, pons, thalamus, cerebellum • Mortality • 50% 30 day mortality • Exam: • sudden HA with focal findings on exam
Risk Factors • Age • Gender (men > women) • Race (blacks > whites) • Prior stroke • Hypertension • Anticoagulant / thrombolytics • Alcohol / cocaine 19 yo with ephedra induced ICH
Less Common Risk Factors • Vascular malformations • Arteriovenous malformations (AVM) • Cavernous angiomas • Intracranial aneurysms • Infections • Cerebral vasculitis • Mycotic aneurysms • Cerebral venous thrombosis
ICH Rate by Age Rate per 100,000 / year Age (years)
Systolic Blood Pressure & Incidence Incidence Rate/100,000 Systolic Blood Pressure (mmHg)
Ethnicity of ICH Risk • Age and sex adjusted rate • U.S. 15 per 100,000 • World wide 10-20 per 100,000 • Higher in African American and Japanese • Rates 13.5 per 100,000 Caucasian 38 per 100,000 AA 55 per 100,000 Japanese
Anticoagulation and Thrombolytic Related Hemorrhage • Warfarin anticoagulation • 6-11 fold increased risk of ICH • Higher levels with increased risk • Most occur in therapeutic range • Thrombolysis and Symptomatic ICH • 6.4% in thrombolysis treatment group • tPA related hemorrhages typically lobar • 20% occur outside area of infarct • 0.6% in placebo group
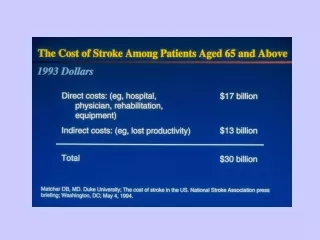
Mortality and Morbidity • Estimated lifetime cost $123,565 • Of the 37,000-65,000 ICH per year • 35-52% were dead at 1 month • 50% of deaths occurred within 48 hours • 10% independent at 30 days • 20% independent at 6 months
30 Day Outcome of ICH No. cases Modified Oxford Handicap Scale
Clinical Presentation • Symptoms and signs • 82% change in mental status • >75% hemiparesis/plegia • 63% headache • 22% vomiting • 2/3 progression of symptoms, 1/3 maximal at onset
Clinical Presentation by Location • Lobar • Headache (headache location related to ICH site) • Motor, sensory deficit, or VF deficits (not all) • Deep • Unilateral motor, sensory, VF loss • Aphasia (D) or neglect (ND) • Cerebellum • Nausea, vomiting, ataxia, coma • Pontine • Coma, quadriplegia, pinpoint pupils
ICH Progression • Symptoms often progress, associated with ICH growth • 26% with 33% or greater growth in 1 hour • 12% with 33% or greater growth 1-20 hours • This gives us a window of therapeutic opportunity
Prognostic Information • Volume of hemorrhage • Clinical presentation • Intraventricular extension (Kothari, Stroke)
Hematoma Volume Calculation • Formula for volume of an ellipsoid • 4/3Л (A/2)(B/2)(C/2) • Simplified ABC/2
Prognosis • Worse • Volume > 60 cm3 and GCS < 9 • 91% dead at 30 days • Patients with volume over 30 cm3 only 1 / 71 independent at 30 days • Intraventricular extension • Better • Volume < 30 cm3 and GCS 9 or higher • 19% dead at 30 days (Broderick, Stroke)
Pathophysiology • Initial hemorrhage into surrounding tissues causes: • Cytotoxic and vasogenic edema formation in the perihematomal parenchyma • Neurotoxicity from released serum proteins • Elevated intracranial pressure due to • Hematoma mass effect • Perihematomal edema • Intraventricular extension and hydrocephalus • Results in decreased perfusion
Current Recommendations for Management of Intracerebral Hemorrhage • Emergency Medicine representation • New guidelines due 2005 Edward C. Jauch, MD MS FACEP (Broderick, Stroke 1999) 30
Emergent Evaluation • Baseline labs • CBC, coags, electrolytes • Neuroimaging • CT remains gold standard • Identify ICH • Identify complications (hydrocephalus, herniation) • MRI / MRA • Useful to evaluate for structural abnormalities • AVM, aneurysms • Angiography • Rarely emergently indicated • Identify vascular issues preoperatively in occult ICH
Medical Management • ABC’s • Blood pressure control • ICP management • Hyperventilation • Osmotherapy • No role for glycerol, corticosteroids, hemodilution • Other • Prevention of hyperthermia • Fluid management (CVP at 5-12 mm Hg) • Modifications for age, comorbidities, size, severity, location • Seizure control • Find somebody to take the patient
Blood Pressure Management • No definitive data (yet) • Hypertension very common • MAP > 140 in 34%, > 120 in 78% • Many return to baseline over first 24 hours (Dr. Aninda Acharya, St.Louis University, Internet Stroke Center)
Blood Pressure Management Edward C. Jauch, MD MS FACEP (Broderick, Stroke 1999) 34
Management of Increased ICP • Definition • ICP > 20 mm Hg for > 5 mins • Treatment goal • ICP < 20 mm Hg • CPP > 70 mm Hg • Recommendations • ICP monitoring with GCS < 9 • Management • Osmotherapy • Hyperventilation • Ventricular drainage
Management of ICP Edward C. Jauch, MD MS FACEP (Broderick, Stroke 1999) 36
Seizure Therapy • 25% will have seizure • Much more common if lobar • Most in first 72 hours • Phenytoin is drug of choice • Does not convey life long epilepsy
What can be Fixed? • Stop the bleeding • Until now no option • Remove the blood • Multiple trials without clear impact • Reduce the edema • No treatment yet
Surgical Treatment • Direct evacuation, endoscopic, stereotactic
Surgical Treatment Recommendations • 7000 procedures a year in U.S. despite lack of data • Largest surgical trial negative (in press) • MISTIE trial of stereotactic evacuation with tPA • (3/05) Surgery in 24 hrs, stable clot for 6 hrs (Broderick, Stroke 1999) 40
The Potential Future With Novo 7What Can We Learn From Acute Ischemic Stroke? 41
Time Will Always Mean Brain! (Lancet 2004; 363: 768–74)
Same Chain: No Weak Links • Development: Protocol and pathway development • Detection: Early recognition • Dispatch: Early EMS activation • Delivery: Transport & management • Door: ED triage • Data: ED evaluation & management • Decision: Neurology input, therapy selection • Drug: Thrombolytic & future agents • Disposition: Admission or transfer 43
Door-to-MD: 10 minutes Door-to-Stroke 15 minutes Team notification: Door-to-CT scan: 25 minutes Door-to-Drug: 60 minutes (80% compliance) Door-to-Admission 3 hours NINDS Recs: Same for ICH (NINDS Stroke Symposium 2003)
There Will Be Major Barriers • EM education of disease and treatment • Timely radiology involvement • Access to neurologic expertise • Neurology does not admit ICH • Neurosurgeons won’t rush in • EM will be point person like tPA • Post treatment management • ICU beds • Complications likely to occur early • Cost • Whose cost center • “Drip and ship” model
Who Cares for Patients with ICH? • Shortage of neurosurgeons • Shortage of neurocritical care • Neurologists not experienced with ICH • Emergency Medicine primarily focused on stabilization • Example – Cincinnati • 30% neurosurgical shortage • Nonoperative ICH to neurology • Only 4 of 15 hospitals with neurosurgery coverage • Only 1 level 1 trauma largely due to neurosurgery
Patient care areas Acute stroke teams Written care protocols EMS participation Emergency Department participation Stroke unit* Neurosurgical services** Support services Organizational support Stroke center director Neuroimaging Laboratory Outcome & quality measures CME Potential Solution:Utilize Primary Stroke Centers • Secondary stroke center likely required for most ICH (Brain Attack Coalition, JAMA 2000)
Questions??www.ferne.orgferne@ferne.orgEdward Jauch, MD, MSjauchec@ucmail.uc.edu(513) 558-0474 ferne_acep_2005_jauch_ich_epipath_cd 6/6/2014 8:37:16 AM