Download
1 / 53
530 likes | 803 Vues
Current Management of Intracerebral Hemorrhage. Edward C. Jauch, MD, MS. Assistant Professor Director of Research Department of Emergency Medicine University of Cincinnati College of Medicine Faculty, Greater Cincinnati / Northern Kentucky Stroke Team. Disclosure. Novo Nordisk

E N D
Edward C. Jauch, MD, MS Assistant ProfessorDirector of ResearchDepartment of Emergency MedicineUniversity of Cincinnati College of MedicineFaculty, Greater Cincinnati / Northern Kentucky Stroke Team
Disclosure • Novo Nordisk • Consultant & Site investigator phase III trial • American Heart Association • ASA and ACLS Stroke Guidelines Committee • Various AHA Committee • National Institutes of Health • Ventricular and hematoma aspiration trials (Genentech providing drug)
Global Objectives • Review epidemiology of ICH • Discuss current treatment recommendations • Review recent developments in ICH treatment • Discuss lessons from acute ischemic stroke
Patient Initial Clinical History • 57 yo male develops sudden onset headache and left sided weakness • Family calls 911 (112, 115, etc) • EMS transport to hospital • Symptoms progress to full hemiplegia • Initial VS: 210 / 120 mmHg, HR 110, R 24
Patient ED Presentation • PMHX: Hypertension for 10 years, hyperlipidemia • SHX: Smoking 30 years • Meds: ACE inhibitor, ASA • ROS: No recent illness or injuries No new medications
Patient ED Presentation • Physical examination: • VS - 220 / 140 mmHg, HR 110, RR 22, T 98.6oF • Neuro (NIHSS = 12) • LOC mildly depressed (GCS 13) • Left facial droop & partial gaze palsy • Dense left hemiplegia • Mild left sensory loss • Speech slurred • Laboratory and ECG normal • Neuroimaging shows
Key Questions • What is your differential diagnosis? • What medical management should be initiated in this patient? • What additional imaging is required? • What laboratory tests should be completed? • What are treatment options and issues?
Lacunar 19% Thromboembolic 6% SAH 13% Cardioembolic 14% Hemorrhagic 26% Ischemic 71% ICH 13% Unknown 32% Other 3% Stroke Subtypes Up to 65,000 ICH per year (Foulkes, NINCDS Stroke Data Bank Stroke, 1988)
ICH Classifications • Primary (80%) • Hypertensive arteriolopathies • Cerebral amyloid angiopathies • Secondary (20%) • Vascular abnormalities • Neoplasms • Coagulation disorders • Anticoagulants or thrombolytic agents • Drugs (cocaine, ephedra, etc) • Trauma
Location • Lobar • Associated with amyloid angiopathy • Nonlobar • Due to hypertension • Cerebellar • Brain stem Cortex Thalamus Basal ganglia Pons Cerebellum
Clinical Presentation • Symptoms and signs • 82% change in mental status • >75% hemiparesis/plegia • 63% headache • 22% vomiting • Symptoms • 2/3 with progression of symptoms • 1/3 maximal at onset (Brott, Stroke 1997;28:1-5)
Clinical Presentation by Location • Lobar • Headache (headache location related to ICH site) • Motor, sensory deficit, or VF deficits (not all) • Deep • Unilateral motor, sensory, VF loss • Aphasia (D) or neglect (ND) • Cerebellum • Nausea, vomiting, ataxia, coma • Pontine • Coma, quadriplegia, pinpoint pupils
Primary Risk Factors • Vascular malformations • Moyamoya / aneurysms • Infections • Vasculitis • Mycotic aneurysms • Cerebral venous thrombosis • Genetic • Apolipoprotein E ε4 • Age • Hypertension • Alcohol intake • Gender (M > F) • Race • Smoking • Diabetes
Pathophysiology • Initial hemorrhage into tissues causes: • Cytotoxic and vasogenic edema formation • Mediators: MMP-9, inflammatory response, blood degradation products • Elevated intracranial pressure due to: • Hematoma mass effect • Perihematomal edema • Intraventricular extension and hydrocephalus • Decreased regional perfusion and herniation
ICH Progression • Symptoms often progress, associated with ICH growth • Within 3 hours from onset: • 26% with 33% or greater growth in next 1 hour • 12% with 33% or greater growth 1-20 hours (Brott, Stroke 1997;28:1-5)
Prognosis • Worse • Volume > 60 cm3 and GCS < 9 • 91% dead at 30 days • Patients with > 30 cm3 • 1 / 71 independent at 30 days • Other: age, seizures, intraventricular extension • Better • Volume < 30 cm3 and GCS 9 or higher • 19% dead at 30 days (Broderick, Stroke 1993;24:987- 93)
28 mL 43 mL (Image courtesy T. Brott, MD)
Hematoma Volume • Formula for volume of an ellipsoid • 4/3π (A/2)(B/2)(C/2) • Simplified A*B*C / 2 C B A (Kothari, Stroke 1996;27:1304-5)
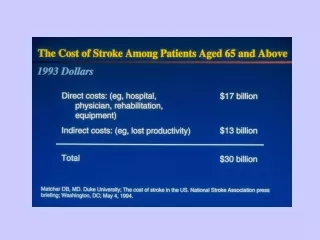
Mortality and Morbidity • Outcome: • 35-52% dead at 1 month • 50% of deaths within 48o • 10% independent at 30 days • 20% independent at 6 months • Lifetime ICH cost $125K # patients Modified Oxford Handicap Scale (Broderick, Stroke 1993;24:987- 93)
Current Recommendations for Management of Intracerebral Hemorrhage New guidelines due 2005 (Broderick, Stroke 1999;30(4):905-15) Edward C. Jauch, MD MS FACEP
Emergent Evaluation • Baseline labs • CBC, coagulation parameters, electrolytes • Neuroimaging • CT remains gold standard • Identify ICH and complications (hydrocephalus, herniation) • MRI / MRA • For structural abnormalities (AVM, aneurysms) • Angiography • Rarely emergently indicated, identifies vascular issues
ICH Management • Immediate stabilization (ABC’s) • Supportive medical care • Frequent comorbidities • Neurologic specific care • Hemorrhage specific interventions
Medical Management • ABC’s • Maintain oxygen saturation ≥92% • Rapid sequence intubation • Medical management • Prevention of hyperthermia (<37.5oC) • Glycemic control (<10 nmol/L) • Coagulopathy correction (FFP, vitamin K) • No glycerol, corticosteroids, hemodilution • Secondary complication prevention (EUSI, Cerebrovasc Dis 2003;16:311-318)
Blood Pressure Management • Hypertension very common • MAP > 140 in 34%, > 120 in 78% • Many ‘normalize’ over first 24 hours • General goals • Maintain MAP < 130 mmHg with history of hypertension • Prevent hypotension (SBP < 90 mmHg) • Maintain: • Cerebral perfusion pressure (CPP=MAP-ICP) CPP > 70 mmHg • Central venous pressure from 5-12 mmHg • Optimal blood pressure still to be determined
Blood Pressure Management • For now - • Common agents • Labetalol • Nicardipine • Nitroprusside • (theoretical risk of • increasing ICP) • New data suggest SBP < 150 mm Hg (Broderick, Stroke 1999;30(4):905-15) (Ohwaki, Stroke 2004;35:1364-1367)
Management of ICP • Definition • ICP > 20 mm Hg for > 5 minutes • Treatment goal • ICP < 20 mm Hg and CPP > 70 mm Hg • Recommendations • ICP monitoring with GCS < 9 • Management • Patient positioning • Osmotherapy • Hyperventilation • Ventricular drainage
Management of ICP • Osmotherapy • Mannitol 0.25-0.5 g/kg every 6 hours up to 5 days • Target mOsm < 310 mmol/L • Hyperventilation • Tidal volume of 12-15 ml/kg • Target pCO2 30-35 mm Hg • Neuromuscular paralysis • Nondepolarizing agents (Broderick, Stroke 1999;30(4):905-15)
Seizures • More common in ICH than you think • Over 25% will seizure (vs 6% for ischemic stroke) • Much more common if lobar • Focal with secondary generalization • Most in first 72 hours • Treatment • Phenytoin (minimizes sedation) • Does not convey life long epilepsy (Vespa, Neurology 2003;60:1441-6)
What can be Fixed? • Stop the bleeding • Until now no option • Remove the blood • Multiple trials without clear impact • Reduce the edema • No treatment yet
Surgical Treatment • Direct evacuation, endoscopic, stereotactic
Surgical Treatment Recommendations • 7000 procedures a year in U.S. despite lack of data • STICH: Largest surgical trial without general benefit (Mendelow, 2005;365:387-97) (Broderick, 1999;30(4):905-15)
Hemostatic Therapy • Few late studies (mostly in SAH*) • Aminocaproic acid • Tranexamic acid* • Ultra-early studies • rFVIIa • Pilot (n=48) • F7ICH-1371 (n=399) • Phase III (n=675) ongoing (Mayer, Stroke 2005;36:74-79) (Mayer, NEJM 2005;352:777-785)
≤ 60 mins Placebo N = 100 rFVIIa 40 µg/kg N = 100 rFVIIa 80 µg/kg N = 100 rFVIIa 160 µg/kg N = 100 Study Design < 3 hours 24-72 hours 90 days • 2° Efficacy • Mortality • mRS • Barthel Index • E-GOS • NIHSS • GCS • Euro-QOL CT Baseline CT 24 h CT 72 h Patients presenting with stroke-like symptoms 1° Efficacy Percent change in ICH volume at 24 hours Baseline CT scan • Safety • Adverse events until discharge • Serious adverse events until day 90 • Exacerbation of edema 20 Countries 73 Trial Sites (Mayer, NEJM 2005;352:777-785)
% 70 65 60 55 50 45 40 35 30 25 20 15 10 5 0 -5 -10 -15 -20 Estimated Mean Percent Change in ICH Volume at 24 Hours Percent Change in ICH Volume by Treatment % 70 52% RR 62% RR 45% RR 65 60 55 50 45 40 35 30 29% * 25 20 16% 14% 14% 15 11% 10 5 0 -5 -10 -15 -20 CombinedTreatment Groups Placebo 40 µg/kg 80 µg/kg 160 µg/kg Treatment Groups *Combined treatment groups vs placebo: P = 0.0112. (Mayer, NEJM 2005;352:777-785)
Modified Rankin Scale at Day 90 0–1 no significant disability 160 µg/kg 2–3 slight to moderate disability 80 µg/kg 4–5 moderately severe to severe disability 40 µg/kg Placebo 0% 20% 40% 60% 80% 100% 6 dead* *29% vs 18% rFVIIa vs placebo, RRR 38%, Chi-square test; P = 0.02 (Mayer, NEJM 2005;352:777-785)
Thromboembolic SAEs Frequency of Thromboembolic SAEs • Arterial thromboembolic SAEs (myocardial ischemia 7 and cerebral infarction 9) with rFVIIa treatment (5%) vs placebo (0%), P = 0.01 • Fatal or disabling thromboembolic SAEs in 2% of rFVIIa-treated patients compared with 2% in the placebo group • Nonsignificant dose trend in events (P = 0.12) (Mayer, NEJM 2005;352:777-785)
Potential Future Tools • Medical therapies • Optimizing blood pressure (ATACH) • Tight glycemic control (THIS) • Neuroprotectives (CHANT, Fast-MAG, hypothermia) • Ultra-early hemostatic therapy (rFVIIa) • Surgery • Surgical patient selection and new approaches • Stereotactic evacuation with tPA • Intraventricular evacuation with fibrinolysis (ITT, DITCH)
Time Will Always Mean Brain! • ICH continue to expand • Early medical management essential • Early coagulation correction critical (drip and ship) • Hemostatic therapy may work best early (Lancet 2004; 363: 768–74)
Same Chain: No Weak Links • Development: Protocol and pathway development • Detection: Early recognition • Dispatch: Early EMS activation • Delivery: Transport & management • Door: ED triage • Data: ED evaluation & management • Decision: Neurologic input, therapy selection • Drug: Thrombolytic (hemostatic) agents • Disposition: Admission or transfer
Door-to-MD: 10 minutes Door-to-”Expert”? 15 minutes Door-to-CT scan: 25 minutes Door-to-Drug: 60 minutes Door-to-Admission 3 hours NINDS RecommendationsSame for ICH? (NINDS Stroke Symposium 2003)
There May Be Major Barriers • Education • Timely radiology involvement • Access to neurologic expertise • Post treatment management • Availability of ICU beds • Complications occur early • Resources and cost
ED Treatment & Patient Outcome • Patient’s GCS declined to 11 over 48o • Mild edema & shift seen on 48o CT • Blood pressure managed with labetalol • Patient required inpatient rehab • Moderately disabled at 3 months but at home
Key Learning Points • ICH is a dynamic process • Critical management frequently required and required early • General management impacts outcome • Targeted therapies time dependent • Hemostatic therapies may play a role if administered early • Surgery for selected cases
Questions?? www.ferne.orgferne@ferne.orgEdward C. Jauch, MD, MSedward.jauch@uc.edu ferne_2005_aaem_france_jauch_ich_fshow.ppt 8/29/2005 1:45 AM
Ethnicity of ICH Risk • Age and sex adjusted rate • U.S. 15 per 100,000 • World wide 10-20 per 100,000 • Rates: 13.5 per 100,000 Caucasian38 per 100,000 African Americans 55 per 100,000 Japanese
ICH Rate by Age Incidence rate / 100,000 per year