Chapter 41 Tetracyclines and chloramphenicol
230 likes | 480 Vues
Chapter 41 Tetracyclines and chloramphenicol. Department of pharmacology Liu xiaokang( 刘小康) 2010,3. Common properties of tetracyclines. Members: Tetracycline, Doxycycline, Minocycline, Demeclocycline, Methacycline. Structure:. Antibacterial activity:

Chapter 41 Tetracyclines and chloramphenicol
E N D
Presentation Transcript
Chapter 41 Tetracyclines and chloramphenicol Department of pharmacology Liu xiaokang(刘小康) 2010,3
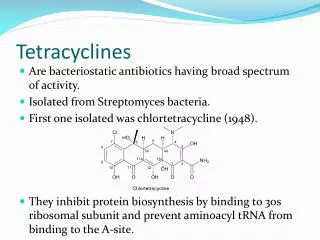
Common properties of tetracyclines • Members: • Tetracycline, Doxycycline, Minocycline, Demeclocycline, Methacycline.
Antibacterial activity: • Broad-spectrum bacteriostatic antibiotics. Include G+ and G– aerobe and anaerobe, ricketts organism, spirochete, mycoplasma, chlamydia and some protozoan. But no activity to Enterococci, Protures and Pseud. aeruginosa.
Mechanisms: • (1) Sensitive bacteria can pump tetracyclines into the cell by energy dependent system; (2) bind to 30S ribosomal subunit at a site that blocks binding of charged tRNA to the "A" site of the ribosome; (3) Tetracyclines can inhibit mammalian protein synthesis, but because they are "pumped" out of most mammalian cells do not usually reach concentrations needed to significantly reduce mammalian protein synthesis.
Pharmacokinetics: • Primarily PO. F varies widely with drug & effect of food. F = 90 to 100%: doxycycline and minocycline; F=58 to 77%: Others. Food decreases: Insoluble chelates -- Ca++, Al+++, Mg++ ; Milk?, Antacids? Some laxatives have Mg++. Distribution: most tissues and fluid, especial bind to Ca++ and sedimentate in bones and teeth. Elimination: Both renal and biliary. Significant enterohepatic circulation.
Clinical uses: • (1) First choice for treatment of rickettsial infections, eg. exanthematous, Q fever and Rocky Mountain Spotted Fever and acariasis; (2) Chlamydia infections, eg. Psittacosis (Chlamydia psittaci); (3) Mycoplasmas infection; (3) Spirochete infection, recurrent fever. (4) bacterial infection: First choice for treatment of cholera, and Brucella infection.
Adverse reactions: • (1) Gastric mucosa, cramps, burning, nausea, vomiting. Can add food if using minocycline or doxycycline; (2) superinfection; (3) Brown discoloration of teeth especially if given during formative stages and deformation of bone; (4) Liver Toxicity, May impair hepatic function, especially during pregnancy and in patients with pre-existing hepatic insufficiency when high doses are given IV; (5) Photosensitivity, Especially demeclocycline. (6) Vestibular reactions, dizziness, vertigo, nausea, and vomiting, If using minocycline or doxycycline at high doses.
Resistance: • Significant resistance, but still useful. Cross-resistance within the group is significant Three primary resistant mechanisms: • (1) Decreased intracellular concentration: (a) Plasmid-borne transporter pumps drug out. Because of multi-valent plasmids, tetracycline resistance is often a marker for resistance to other drugs, e.g., aminoglycosides, sulfonamides, and chloramphenicol; (b) Decreased penetration in some bacteria; • (2) Production of proteins that interfere with tetracycline binding to ribosomes; • (3) Enzymatic inactivation.
Tetracycline: • Similar with doxycycline in clinical use, but more adverse reaction
Doxycycline: • The major clinic used tetracycline; it is fast effecting, high efficacy and long-term duration. • Used for all indications of tetracyclines with less adverse reactions, usually gastrointestinal reaction.
Minocycline: • Similar with doxycycline.
Cloramphenicol • Structure:
Antimicrobial activity: • Broad spectrum. Effect on G+ and G– bacteria, ricketts organism, spirochete, chlamydia, mycoplasma.
Mechanism: • (1) blocks proper binding of aminoacyl moiety to "A" site. Failure to properly align prevents Peptidyl transferase enzyme from transferring the growing chain from the "P" site to the bound charged tRNA in the "A" site. This stops protein synthesis. • (2) Chloramphenicol does inhibit mitochondrial ribosomal protein synthesis because these ribosomes are 70S, the same as those in bacteria. It does not bind to the 80S mammalian ribosomes. This may be responsible for the dose related anemia caused by chloramphenicol.
Pharmacokinetics: • Rapidly absorbed. Well distributed, in CSF can reach 60% (45-90%) of plasma concentration in presence or absence of meningitis. 90% Eliminated by glucuronyl transferase (Liver enzyme)
Clinical uses: • Resembles tetracyclines, except More serious hazard so limit use (The risk of aplastic anemia does not contraindicate the use of chloramphenicol in situations in which it is necessary; however, it emphasizes that the drug should never be employed in undefined situations or in diseases readily, safely, and effectively treatable with other antimicrobial agents)
(1) More likely for CNS than tetracyclines, Very effective in Haemophilus influenzae meningitis, but several third generation cephalosporins have replaced CAP as initial therapy when this organism is suspected. (cefotaxime, ceftriaxone, and ceftizoxime); • (2) Universally active vs anaerobic bacteria, rickettsiae, chlamydia, mycoplasma.
Adverse reaction: • (1) aplastic anemia; (2) Gray Baby Syndrome; (3) Reversible, dose-related hematologic toxicity; (4) others.
Resistance: • Plasmid borne acetyltransferase is primary mechanism.
Drug interaction: • Inhibits hepatic microsomal cytochrome P450 enzymes, Depresses hepatic biotransformation of other drugs prolong half-lives of many drugs, e.g. dicumarol, phenytoin, tolbutamide and chlorpropamide. • (The end)