Comprehensive Overview of Abdominal Herniae: Types, Complications, and Management
This detailed guide explores abdominal herniae, defined as the protrusion of organs through their surrounding walls, focusing on common types such as inguinal, umbilical, femoral, and incisional hernias. It discusses the etiology of hernias, risk factors including congenital weakness and trauma, and emphasizes the importance of diagnosis to prevent serious complications like strangulation and bowel obstruction. Additionally, it covers the anatomy of the inguinal region, differentiating between direct and indirect inguinal hernias, and outlines the symptoms, signs, and surgical management options.

Comprehensive Overview of Abdominal Herniae: Types, Complications, and Management
E N D
Presentation Transcript
ABDOMINAL HERNIAE LIDIA IONESCU 3rd.Surgical Unit
DEFINITION • HERNIA= a protrusion of an organ through its containing wall • Herniation of the muscle through its fascial covering • Herniation of the brain through a fracture of the skull • Herniation of an intra-abdominal organ through a defect in the abdominal wall, pelvis or diaphragm-the term “hernia” is used to describe an abnormal opening in a patient’s muscle that will allow tissue or organs to pass through the opening in the muscle
Abdominal herniae • Before an organ can herniate through its retaining wall – there must be a weakness in that wall: • Normal- related to the anatomical configuration • Abnormal weakness - congenital abnormality - acquired as a result of trauma or disease
Types of hernias • Common types: • Inguinal • Umbilical • Femoral • Incisional hernia • Less common types: • Epigastric • Spigelian • Obturator
BE AWARE • FAILURE TO DIAGNOSE ANY TYPE OF STRANGULATED HERNIA COMMON OR RARE MAY LEAD TO THE PATIENT’S DEATH
Complications • Irreducibility- bowel obstruction- incarcerated bowel • Strangulation – bowel obstruction + necrotic bowel
Relation to gender • Inguinal hernia is common in men • Femoral hernia is more common in women
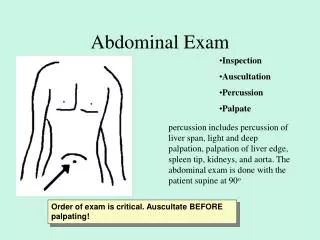
Certain physical signs • Occur at weak spots in the abdominal wall • Reduce on lying down or with direct manual pressure • Expansive cough impulse
Etiology • Defects in the abdo wall: • Structures pass through: indirect inquinal, epigastric • Muscles fail to overlap: spigelian, lumbar • No muscles, only scar tissue: umbilical hernia • Loss of tissue strength: • Direct inquinal hernia • Increased intra-abdo pressure • Trauma
Inguinal hernia • This type of hernia accounts for the vast majority of hernia surgical repairs. • An inguinal hernia is located in the inguinal region of the body where the thigh meets our pelvis. • The most common types of inguinal hernias are either direct or indirect hernias and these are found more often by far in men rather than women.
Inguinal and femoral hernia • It is possible to develop three types of hernia in, or close to the inguinal region: direct inguinal; indirect inguinal; femoral. • Each opening (the deep and superficial inguinal rings) is visible and “protected” by two of the muscle layers. • The muscles and their aponeuroses were clearly defined and two of them (internal oblique and transversus abdominis) could be seen arching over the canal to form its roof and then its posterior wall (conjoint tendon).
Descriptive terms • Reducible hernia- hernia content can be pushed back into the abdomen • Irreducible hernia-incarcerated hernia- hernia content cannot be pushed back • Obstructing hernia- hernia containing a loop of bowel that is kinked and therefore obstructed • Strangulated hernia-the tissue contained in the hernia is ischemic due to interruption of the blood supply • Sliding hernia-when the wall of the hernia sac in part formed by the wall of another intra-abdominal organ( colon, bladder) • Richter’s hernia-one side of the bowel wall is trapped in the hernia
Complications • Intestinal obstruction- a loop of bowel passes through the abdo. wall defect and becomes mechanically obstructed. • Intestinal strangulation with gangrene/perforation – vascular pedicle to the herniated loop of bowel is also interrupted
Inguinal herniaAnatomy of the inguinal region • Superficial inguinal ring- triangular defect in the aponeurosis of the EOM and the pubic crest • Deep inguinal ring- an oval opening in the fascia transversalis, 1,3 cm. above the mid-inguinal ligament. • Medially- inf. epigastric vessels • Inguinal canal- oblique passage through the lower part of the anterior abdominal wall • Spermatic cord • Round ligament
Inguinal canal • 1. Inguinal canal • 2. Spermatic cord • 3. Testis • 4. Uterus • 5. Round ligament • 6. Lymph vessels • 7. Superficial inguinal nodes • 8. Deep inguinal ring • 9. Superficial inguinal ring
Inguinal canal • 4 cm. long, between deep and superficial rings • Anterior wall- EOM aponeurosis • Inferior wall- inguinal ligament • Superior wall- conjoint tendon • Posterior wall- transversalis fascia • Hesselbach’s triangle- within the posterior wall: inf.epi.art.- inguinal lig.-lateral border of the rectus sheath
Types of inguinal herniae • Indirect inguinal herniae • Passes through the deep inguinal ring, down the inguinal canal • May extend into the scrotum • 5 times commoner than direct hernia • Direct inguinal hernia • Passes through the Hesselbach triangle • Posterior to the spematic cord • Does not pass into the scrotum • Less often associated with strangulation
Symptoms and signsInguinal hernia • Gender- all ages • Occupation- heavy works • Local symptoms- dragging sensation in the groin • Systemic symptoms- obstructive hernia- vomiting, distension, colicky abdominal pain, absolute constipation
Inguinal herniaPhysical examination • Position- above the inguinal ligament • Tenderness- if strangulated • Shape- “pear-shaped” with the “stalk” at the external inguinal ring • Composition- soft-gut, firm-omentum. • Cough impulse • Reducibility
Inguinal herniaGeneral examination • Look for causes of a raised intra-abdominal pressure: • Chronic bronchitis- caughing • Chronic retention of urine- difficulty in micturition • Chirrhosis - ascites • Intra-abdominal masses Look for signs of intestinal obstruction: - Abdominal distention - Visible peristalsis - High-piched bowel sounds
Inguinal herniaDifferential diagnosis • Femoral hernia • Vaginal hydrocele • Undescended testis • Lipoma
Femoral herniaAnatomy • Femoral canal – space containing lymphatic and fat tissue • Femoral ring: inguinal ligament, Cooper’s ligament, pectineal line, femoral vein
Femoral hernia • Femoral ring is rigid- strangulation more likely • The bulge can be palpated in inguinal crease, below inguinal ligament • Obese patients- difficult to palpate • Think to a complicated femoral hernia in an obese patient with painful femoral area and bowel obstruction symptoms • More common in women • Related with physical effort
Symptoms and signsFemoral hernia • Age - uncommon in kids • Gender -women more affected • Position - below and lateral to the pubic tubercle • Tenderness - not tender unless complicated • Shape and size - spherical, small • Surface - smooth • Reducibility- firm pressure • Cough impulse - tight ring- less likely
Differential diagnosisFemoral hernia • Inguinal hernia • Enlarged lymph nodes • Sapheno-varix • Ectopic testis • Psoas abscess • Lipoma
Umbilical hernia • This type of hernia occurs at the level of the naval and are usually the result of the failure of the abdominal wall defect to close after the patients umbilical cord falls off as an infant. Most of these hernias defects will close in childhood by the age of 3-5. • Remaining umbilical hernias however can enlarge over time and require repair in the adult patient.
Congenital umbilical hernia • 90% of cases, defects are closed by the age of one year • 99% by 2 years of age • Surgery is contraindicated below the age of 3 years
Acquired umbilical hernia • Adult hernia through the umbilical scar • Secondary to a raised intra-abdominal pressure
Umbilical hernia • Congenital umbilical hernia • Acquired umbilical hernia • Para-umbilical hernia
Para-umbilical hernia • Acquired umbilical hernia • Appears through a defect that is adjacent to the umbilical scar
Marked ascites and an umbilical hernia, which had ruptured a few days before the photograph, in a patient with cirrhosis and portal hypertension secondary to hepatitis C.
Spigelian hernia • This type of hernia is a rare form of hernia defect that can occur at the level of the umbilicus but actually lateral to it. • These hernias are often difficult to diagnose