Download

1 / 16
160 likes | 245 Vues
This study examines the early results of the Virginia Coordinated Care Delivery System, evaluating costs, utilization patterns, and the impact on the newly insured poor. By implementing a patient-centered medical home model, the program aims to reduce barriers to care and improve outcomes for underserved populations. Initial evaluation data from 2000 to present show promising trends in lower ED visit rates and increased access to primary care. However, challenges in managing costs and optimizing care delivery persist. This research provides valuable insights into the effectiveness of innovative healthcare programs in addressing the needs of vulnerable populations.

E N D
Early Results of Costs and Utilization, Virginia Coordinated Care Delivery System Wally R. Smith, MD, Donna K. McClish, PhD, Patricia Carcaise-Edinboro, PhD, Gloria Bazzoli, PhD,Alton Hart, MD, MPH, Arline Bohannon, MD,Peter Boling, MD,Sheldon Retchin, MD, MPH, MSHA Virginia Commonwealth University AHRQ MD-10-012
Background • Uninsured • Utilization patterns similar to Medicaid, underinsured • Poor • Lower social support • Less transportation, education, delayed gratification • May use ED rather than PCP • Health Care Reform • Reduces the number of uninsured, underinsured • Of the 46 million uninsured, estimated 32 million will soon be covered • Expands Medicaid program to approximately 16 million newly insured
Do the Newly Insured Poor Change Utilization Patterns? • Not in some studies of providing managed care insurance-like programs to uninsured • Barriers and Weaknesses of previous programs • Short duration • Dose of managed care variable • Little case management • Poor PCP (geographic or time) availability • Few barriers to ED access • Comorbidity mix unfavorable
Virginia Coordinated Care 2000-present • Patient-Centered Medical Home Insurance-like program for uninsured • Uses managed care principles • All patients qualify for the Indigent care program supported by federal DSH and State General funds • Primary care provided by community PCP’s funded by VCUHS profits from commercial plans • FFS and Management fee paid to PCPs in urban communities surrounding VCU • Catchment area within 30 miles of VCU • Patients given card with PCP’s name • Case managers support, assist with ∆’s, • Enrollment files managed by Medicaid HMO owned by VCU Health System
Initial Evaluation of VCC • Lower ED visit rates • Patients saw PCP • VCC off-loaded patients to community physicians • Community physicians happy with management fees • Case management dose small • Short-term evaluation only
How Did VCC Enrollment, Costs, and Utilization Grow from 2003-2005? Utilization? Per Member Per Month (PMPM) Costs? Uptake by community PCP’s? Relative costs?
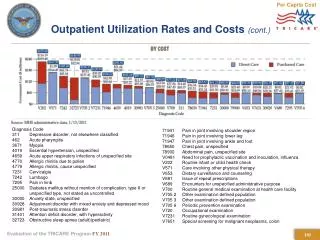
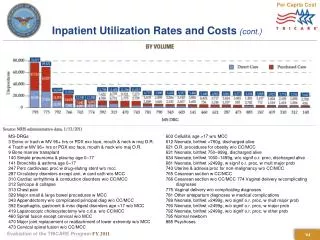
PMPM Costs by Svc Type * Missing ED data for Richmond Community Hospital FY03, all data for FY05 incomplete
Conclusions-1 There was a 12% annual increase, and a 25% increase overall, in VCC enrollment from FY 2003-2005. Simultaneously, community practitioner member months increased 28%. Per member per month costs rose slightly for pharmacy and ED, but were flat for inpatient and outpatient services.
Conclusions-2 Overall, the percentages of VCC pts seeking primary care slightly increased, but so did the percentage w all other visits. Specialty care utilization percentages dropped slightly. Uptake %’s by community primary care mirrored dropoff %’s by VCU primary care. Community primary care PMPM rose, but was more than offset by decreases in university primary care PMPM, leading to a decrease in PMPM for these segments combined. Specialty care PMPM remained flat.
ED PMPM Details * Missing ED data for Richmond Community Hospital FY03, all data for FY05 incomplete