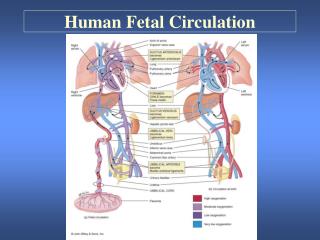
Fetal Circulation
Fetal Circulation. Normal Heart. Cardiovascular Exam in the Child with Heart Murmur Epidemiology. Innocent murmur - 12,050 schoolage children from South Africa, 72% had innocent systolic murmur * Ref - MacLaren et al. Br Heart J 1980;43:67-73
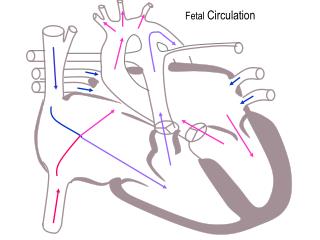

Fetal Circulation
E N D
Presentation Transcript
Cardiovascular Exam in the Child with Heart Murmur Epidemiology • Innocent murmur - 12,050 schoolage children from South Africa, 72% had innocent systolic murmur * Ref - MacLaren et al. Br Heart J 1980;43:67-73 • Heart disease - 0.8% of liveborn babies have congenital heart defect, 0.4% bad enough to detect before 1st birthday * Ref - Samanek et al. Pediatr Cardiol 1989;10:205-211. * Ref - Ferencz et al. Am J Epidemiol 1985;121:31-36
Cardiovascular Exam in the Child with Heart Murmur Features of Innocent Murmurs • Still’s Murmur * Timing: Systolic ejection * Intensity: 1-3/6 * Location: Several cm lateral to LLSB * Pitch: Low * Character: Vibratory * Helpful Maneuvers: Inspiration, standing
Cardiovascular Exam in the Child with Heart Murmur Features of Innocent Murmurs • Pulmonary Flow Murmur * Timing: Systolic ejection * Intensity: 1-3/6 * Location: LUSB * Pitch: Low to medium * Character: Blowing * Helpful Maneuvers: Inspiration, standing
Cardiovascular Exam in the Child with Heart Murmur Features of Innocent Murmurs • Pulmonary Branch Murmur of Infancy * Timing: Systolic ejection * Intensity: 1-3/6 * Location: LUSB, RUSB, to axillae and back * Pitch: Medium * Character: Blowing * Helpful Maneuvers: None
History Dyspnea, cough, “asthma” Exercise Intolerance (child) Feeding Difficulties (infant) DIzziness, syncope Palpitations Chest pain Cyanosis (infant) Physical Exam Height, weight, growth chart BP (upper and lower) Pulses, perfusion Color Liver, spleen Breath sounds Precordial palpation RR, grunt? flare? retract? HR, regular? Cardiovascular Exam in the Child with Heart Murmur The H&P Beyond Auscultation
Physiologic Categories of Congenital Heart Disease • Left-to-right shunt • Right-to-left shunt • Admixture lesions • Obstructive lesions
Imaging CHD • Echocardiography • Cardiac Catheterization • CT • MRI • CXR
Small VSD – Clinical Presentation • Laboratory testing • X-ray – normal • EKG – normal • Echo for anatomic dx • H & P • Asx throughout life • Holosystolic murmur at left mid-to-lower sternal border
Small VSD – Subsequent Course/Complications • Many Close Spontaneously • Usually No Complications • At Risk For Bacterial Endocarditis (e.g. with dental work) When Small VSD Stays Open • Normal Life Expectancy Without Limitations
Small VSD – Treatment Options • Antibiotic Prophylaxis Against Bacterial Endocarditis During Times Of Risk (e.g. with dental work) • Surgical Or Transcatheter Closure Not Indicated
Large VSD – Clinical Presentation • H & P • Respiratory sx • Failure to thrive • Low pitched holosystolic murmur at left lower sternal border • Increased intensity P2 • Diastolic flow rumble @ apex • Increased precordial activity • Laboratory testing • X-ray – cardiomegaly with increased pulmonary vascularity • EKG – LAE, LVH, BVH • Echo for anatomic dx
Large VSD – Subsequent Course/Complications • Can Get Smaller Or Close Spontaneously • Recurrent Pneumonia • Chronic Respiratory Sx, Exercise Intolerance • Failure to Thrive • Pulmonary Vascular Obstructive Disease (Eisenmenger’s) • Endocarditis Risk • Premature Death
Large VSD – Treatment Options • Diuretics • Afterload Reduction • Inotropes • Prophylaxis Against Endocarditis • Surgical Closure • Transcatheter Occlusion (Experimental)
ASD – Subsequent Course/Complications • Right Heart Failure • Pulmonary Hypertension • Atrial Arrhythmias • Premature Death
ASD – Treatment Options • Surgical Closure • Transcatheter Occlusion
PDA in the Premature Neonate – Clinical Presentation • H & P • Respiratory sx, exacerbation of RDS • Failure to thrive • Not much murmur • Bounding pulses • Increased precordial activity • Laboratory testing • X-ray – cardiomegaly with increased pulmonary vascularity • EKG – Not very helpful • Echo for anatomic dx
PDA in the Premature Neonate –Subsequent Course/Complications • Prolonged Ventilator Course • Intraventricular Hemorrhage • Necrotizing Enterocolitis • Contributor To Neonatal Mortality & Morbidity
Large PDA in the Older Child – Clinical Presentation • H & P • Respiratory sx, exercise intolerance • Continuous murmur @ left upper sternal border • Wide pulse pressure, bounding pulses • Increased LV impulse • Laboratory testing • X-ray – cardiomegaly with increased pulmonary vascular marking • EKG – LVH, LAE • Echo for anatomic dx
Small PDA in the Older Child – Clinical Presentation • H & P • Asymptomatic • Continuous murmur @ left upper sternal border • Laboratory testing • X-ray – usually normal • EKG – usually normal • Echo for anatomic dx
PDA - Treatment Options • Antibiotic Prophylaxis Against Bacterial Endocarditis During Times Of Risk (e.g. with dental work) • Indomethacin (Premature Neonates Only) • Transcatheter Closure (Older Than Neonates Only) • Surgical Ligation
Classification of Congenital Heart Disease – Right-to-Left Shunts • Definition: deoxygenated blood is delivered to the systemic arterial circulation without first passing through the lungs • Examples: tetralogy of Fallot; transposition of the great arteries
Tetralogy of Fallot – Clinical Presentation • H & P • Cyanosis (may not be evident at birth) • Systolic ejection murmur at left upper sternal border • Increased precordial activity • Digital clubbing (late) • Exercise intolerance/ Squatting behavior (late) • Laboratory testing • X-ray – often normal, can show “coeur en sabot”, upturned apex, narrow mediastinum, decreased pulmonary vascularity, right aortic arch • EKG – RVH, RAD, less often RAE • Echo for anatomic dx
Tetralogy of Fallot – Subsequent Course/Complications • Chronic Progressive Cyanosis • Polycythemia, Stroke, Brain Abscess • Exercise Intolerance • Hypercyanotic Episodes • Endocarditis Risk • Premature Death
Tetralogy of Fallot – Treatment Options • Prophylaxis Against Endocarditis • Surgical Repair • Palliative Systemic To Pulmonary Arterial Shunt (Blalock-Taussig) • Palliative Balloon Pulmonary Valvuloplasty Occlusion (Experimental) • Beta Blockade (Historical Interest)
Transposition of the Great Arteries – Subsequent Course/Complications • Progressive Hypoxemia • Acidosis • Death in Infancy
Transposition of the Great Arteries – Treatment Options • Prostaglandin E1 • Balloon Atrial Septostomy • Arterial Switch Operation • Atrial Baffle Operations (e.g. Senning, Mustard) – Historical Interest
Classification of Congenital Heart Disease – Obstructive Lesions • Definition: blood is impeded by narrowed valves, arteries, or veins, anywhere in the systemic or pulmonary circulations • Examples: pulmonary valve stenosis; aortic valve stenosis; coarctation of the aorta
Pulmonary Valve Stenosis – Clinical Presentation • H & P • Asymptomatic if mild/moderate • Exercise intolerance if severe • Systolic ejection murmur @ left upper sternal border • Systolic ejection click • Increased right ventricular impulse if moderate/severe • Laboratory testing • X-ray – normal heart size, prominent MPA, normal distal pulmonary vascularity • EKG – RVH if more than mild • Echo for anatomic dx and assessment of severity