Using Blood Gases
This presentation by Dr. Jonathan R. Goodall at the M62 Coloproctology Meeting provides an in-depth overview of arterial blood gases (ABGs) and their interpretation in Intensive Care Units (ICUs). It covers the basics of ABGs, including normal values, acid-base status, and the significance of oxygenation parameters. Clinical examples are discussed, focusing on how to effectively interpret ABG results and their implications for patient management. Emphasis is placed on the importance of context, highlighting potential treatment-related complications.

Using Blood Gases
E N D
Presentation Transcript
Using Blood Gases Dr. Jonathan R. Goodall M62 Coloproctology Meeting 2nd April 2004
Teaching Grandma to suck eggs… JRG Hope Hospital April 2004
Introduction • The necessary basics • Clinical examples of ABG use in ICU • Newer considerations in interpretation of acid-base disturbances JRG Hope Hospital April 2004
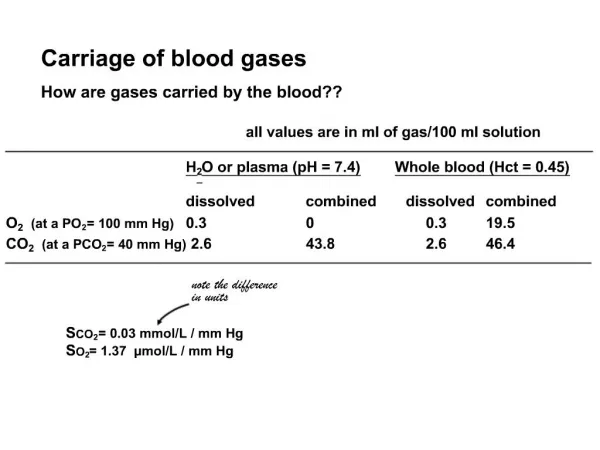
The Basics - Normal Values • pH 7.35 - 7.45 H+ 35- 45 nmol.l-1 • pCO2 4.5 - 6 kPa • pO2 11 -14 kPa • Actual HCO3 22-26 mmol.l-1 • Standard HCO3 22-26 mmol.l-1 • Base Excess +/- 2.0 • SaO2 ≥ 95 % JRG Hope Hospital April 2004
Oxygenation PaO2 ? SaO2 + Hb more important Interpret only with knowledge of FiO2 The Basics - Interpretation JRG Hope Hospital April 2004
Acid-Base Status pH pCO2 HCO3 (actual or standard) Base Excess Oxygenation PaO2 SaO2 + Hb more important? Interpret only with knowledge of FiO2 The Basics - Interpretation JRG Hope Hospital April 2004
H2O + CO2 H2CO3 H+ + HCO3- JRG Hope Hospital April 2004
H2O + CO2 H2CO3 H+ + HCO3- JRG Hope Hospital April 2004
The Basics - Standard Bicarbonate • The amount of bicarbonate that would be present if: • PCO2 was 5.3 kPa • Temp 37°C • Blood fully oxygenated • At sea level JRG Hope Hospital April 2004
The Basics - Base Excess (Deficit) • The amount of base that needs to be added to or subtracted from each litre of blood (ecf) to return the pH to a value of 7.4 at: • pCO2 5.3 kPa • Temp 37°C JRG Hope Hospital April 2004
Ivor Lewis Oesophagectomy • 54 year old lady • No significant PMH • 7 hour procedure • Initial post op period stable JRG Hope Hospital April 2004
Cellulitis (?) • 75 year old lady • Established atrial flutter • Admitted with spreading cellulitis right calf • Hypotension unresponsive to fluids (and dobutamine!) JRG Hope Hospital April 2004
Initial ABGs JRG Hope Hospital April 2004
Hyperchloraemic acidosis • Base deficit traditionally used as marker for metabolic acidosis • Appropriate fluid resuscitation should decrease base deficit • Chloride rich solutions (0.9% NaCl) can potentiate metabolic acidosis www.anaesthetist.com/icu/elec/ionz/Stewart • If base deficit persists despite ‘adequate’ fluids in an otherwise well patient, check [Cl-]! JRG Hope Hospital April 2004
Summary • Arterial blood gases can be used to guide therapy • Must be interpreted in the light of the clinical setting • Look at acid–base disturbances, then oygenation with FiO2 • Remember the possibility that treatment may cause problems! JRG Hope Hospital April 2004