Electrolytes and Shock
430 likes | 626 Vues
Electrolytes and Shock. Janis Rusin APN, MSN, CPNP-AC Pediatric Nurse Practitioner Lurie Children’s Transport Team. Objectives. Discuss the function of each of the following electrolytes; sodium, potassium, magnesium, c alcium and phosphorus Discuss the causes of electrolyte derangements

Electrolytes and Shock
E N D
Presentation Transcript
Electrolytes and Shock Janis Rusin APN, MSN, CPNP-AC Pediatric Nurse Practitioner Lurie Children’s Transport Team
Objectives • Discuss the function of each of the following electrolytes; sodium, potassium, magnesium, calcium and phosphorus • Discuss the causes of electrolyte derangements • Discuss the definition and management of compensated and decompensated shock • Discuss the types of shock • Identify the interventions on transport to manage electrolyte derangements and shock
Body Fluids and Total Body Water • Bodily fluids are divided between two compartments • Intracellular Fluid (ICF)-Fluid within the cells • Extracellular Fluid (ECF)-All the fluid outside of the cells including the bloodstream • Subdivided into Interstitial and Intravascular Fluids • Water travels back and forth between these compartments • Primarily driven by osmosis • The integrity and proper functioning of the cell membranes also contribute to the movement of water • The amount of the fluid in both compartments together is referred to as the Total Body Water (TBW)
Total Body Water • Infants have the highest percentage of TBW • Adults have the least • The higher the percentage of body fat, the lower the percentage of TBW • Males have more TBW than females
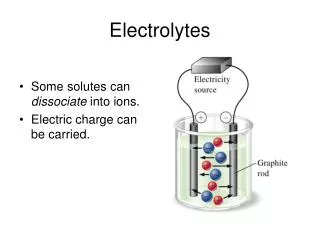
Electrolytes • An electrolyte is an element or compound that when dissolved in water dissociates into ions and conducts an electrical current • Sodium primarily exists in the ECF and maintains the osmotic balance of the ECF • Potassium primarily exists in the ICF and maintains the osmotic balance of the ICF • These two electrolytes tend to repel each other. • If one increases in one space the other will be driven to the opposite space • Water follows salt
Sodium • My Favorite condiment! • Maintains the osmolality of the ECF • Interacts with potassium and calcium to maintain electrical nerve impulses • Sodium balance is regulated by the hormone Aldosterone • Aldosterone: • Produced by the adrenal cortex • Acts on the distal tubule to reabsorb Na and H2O • Potassium is then excreted from the Distal tubule
Sodium Imbalance • Hypernatremia • Serum Na > 147mEq/L • Dehydration/hypovolemia • Diabetes Insipidus • Hyperaldosteronism • Hypertension • Iatrogenic • Excessive administration of hypertonic saline solutions • Cushings syndrome • Increased secretion of ACTH • Also stimulates aldosterone production
Hypernatremia • Symptoms • Thirst • Dry mucous membranes • Weight loss • Concentrated urine (except in DI) • Tachycardia • Hypotension-due to volume depletion • Management • Determine the cause • Rehydrate with isotonic free water solution • D5W • Monitor Na levels closely
Hyponatremia • Serum Na < 135mEq/L • Diuretics • SIADH • Dilutionalhyponatremia • Excess water intake • Dilution of infant formula • Administration of mannitol • Causes osmolar shifts of free water into cells leading to cellular edema • Symptoms: • Lethargy, Headache, Seizures, Weight gain, Edema, Ascites
Hyponatremia • Management • Determine the cause • Fluid restrictions • Sodium correction with hypertonic solution (3% NaCl) • Determine the sodium deficit and replaces slowly • Symptomatic patients • Replace 3-5 mEq/L/hr • Asymptomatic patients • Replace 0.5-1 mEq/L/hr • Na deficit = (0.6) X Wt (kg) X (Na-goal – Na-actual)
Sodium correction • Patient with serum sodium of 125 mEq/L who weighs 20 kg • 0.6 X 25 X (136 – 125) = 165 mEq/L • 3% Saline contains 513 mEq/L which is 0.513 mEq/ml • Replace 5mEq/L/hr • 165 divided by 5 = 33 hours • 5mEq/hr divided by 0.513mEq/ml = 9.7 ml/hr for 33 hours
Potassium • Major intracellular electrolyte • Maintains ICF osmolality • Maintains the resting cell membrane potential • Along with Na, contributes to the electrical conduction of nerve impulses in cardiac, skeletal and smooth muscle
Hyperkalemia • Serum K level > 5.5 mEq/L • Often caused by movement of K from the ICF to the ECF • Cellular trauma • Burns, Crush injuries • Acidosis • H ions shift into the cells and K shifts out • Change in cell membrane permeability • Insulin deficiency • Renal failure
Hyperkalemia • Management • Calcium Gluconate stabilizes cell membranes in the presence of dangerously high K levels • Should be given to prevent cardiac arrhythmias while K is being corrected • Administration of glucose and insulin • Glucose stimulates insulin production • Insulin drive K back into the cell • Sodium Bicarbonate • Correction of metabolic acidosis • Rectal cation exchange resins • Kayexalate • Not a popular treatment on transport
Magnesium • Major intracellular ion • Mostly stored in muscle and bone • Very small amounts in the serum • Contributes to intracellular enzyme reactions • Protein synthesis • Neuromuscular responsiveness to electrical impulses
Magnesium • Hypermagnesemia • Mg > 2.5mEq/L • Renal Failure • Excess ingestion of Mg antacids • Depressed contraction of skeletal muscles • Depressed nerve function • Hypotension • Bradycardia • Respiratory depression • Hypomagnesemia • Mg < 1.5 mEq/L • Malnutrition/malabsorbtion • Alcoholism • Diuretics • Metabolic acidosis • Increased neuromuscular excitability • Tetany • Ataxia • Nystagmus • Seizures
Calcium • Primarily (99%) located in the bone • In serum, 50% is bound to proteins, 40% is in the free/ionized form • Major cation for the maintaining the structure of bones and teeth • Contributes to blood clotting • Maintains plasma membrane stability and permeability • Contributes to muscle contraction and nerve impulses
Phosphate • Also found primarily in bone • Exists in cells as creatanine phosphate and ATP • Provide energy for muscle contration • Acts as an intracellular buffer to maintain acid base balance within the cell
Calcium and Phosphate • They have a synergistic relationship • If the concentration of one increases, the other decreases • They are regulated by parathyroid hormone, vitamin D and calcitonin • Parathyroid (PTH) is sensitive to Ca levels • When Ca levels are low, PTH is stimulated • PTH stimulates the kidney to reabsorb Ca and excrete PO4 • The kidney also activates Vitamin D which stimulates the absorbtion of Ca from the small intestine • Vitamin D also enhances bone absorption of Ca • In renal failure, Vitamin D is not activated, Ca decreases and PO4 increases
Calcium • Hypocalcemia • Serum Ca < 8.5 mg/dl • Nutritional deficiencies • Inadequate Ca or Vit D intake • Decreased PTH • Symptoms • Confusion • Parasthesia’s • Muscle spasms to hands and feet • Hyperreflexia • Hypercalcemia • Ca > 12 mg/dl • Hyperparathyroidism • Bone Metastasis • Excess Vitamin D • Symptoms • Fatigue/weakness • Bradycardia and heart block • Lethargy • Anorexia • Nausea • Constipation • Kidney stones
Phosphate • Hyperphosphatemia • PO4 > 4.5mg/dl • Chemotherapy resulting in cell destruction • Hypoparathyroidism • Symptoms • Same as Hypocalcemia • Chronically, calcification of lungs, kidneys and joints • Hypophosphatemia • PO4 < 2.0 • Intestinal malabsorption • Vitamin D deficiency • Alcohol abuse • Hyperparathyroidism • Symptoms: • Decreased cellular metabolism • Reduced capacity for oxygen transport (requires ATP) • Bradycardia and MI • Clotting disorders
Shock • Shock is defined as an abnormal condition of inadequate blood flow to the body tissues, with life threatening cellular dysfunction • Basically it is supply and demand: O2 supply is down and demand is up • Remember: CO = HR X SV • Oxygen delivery to the tissues is the product of cardiac output and the oxygen content of arterial blood • Mortality rate varies from 25-50% • Most patients do not die in the initial stages
Shock • Primary cardiac arrest in infants and children is rare • Pediatric cardiac arrest is often preceded by respiratory failure and/or shock and it is rarely sudden • Early intervention and continued monitoring can prevent arrest • The terminal rhythm in children is usually bradycardia that progresses to PEA and asystole • Septic shock is the most common form of shock in the pediatric population • 80% of children in septic shock will require intubation and mechanical ventilation within 24 hours of admission
Organ System Involvement • Cellular • Decreased perfusion leads to anaerobic cellular metabolism • Increased lactic acid production: metabolic acidosis • Increased permeability of cell wall • Fluid shifts • Activation of clotting cascade (DIC) • Failure of the Na/K pump • Impaired glucose delivery
Organ System Involvement • Cardiac: • Decreased preload • Decreased cardiac output • Decreased systemic vascular resistance • Decreased coronary blood flow • Cardiac ischemia • Arrhythmias • Progressive heart failure occurs
Organ System Involvement • Respiratory: • Increased permeability to fluid shifts • Pulmonary edema • Decreased O2 transport • Hypoxia • Acidosis • Lung damage: ARDS
Organ System Involvement • Renal • Decreased renal blood flow • Renin-Angiotension system kicks in • Aldosterone causes Na and water retention • Persistent decreased renal perfusion leads to kidney failure
Organ System Involvement • Neurologic • Cerebral perfusion decreases • Patient becomes obtunded • Vasomotor area of the brain becomes less active • Vascular tone cannot be maintained • Vascular collapse occurs
Types of Shock • Hypovolemic • Cardiogenic • Obstructive • Distributive • Septic • Neurogenic • Anaphylactic
Hypovolemic Shock • Occurs from loss of blood or body fluid volume from the intravascular space • Traumatic injury • Vomiting or diarrhea • Classes of hemorrhage: • Class I: <15% blood loss • Class II:15-25% • Class III: 26-39% • Class IV: >40%
Cardiogenic Shock • Pump Failure • Inability of the heart to maintain adequate cardiac output • SVT, arrhythmias, • Cardiomyopathy • Support ABC’s • Treat the cause
Obstructive Shock • Inadequate cardiac output due to an obstruction of the heart or great blood vessels • Cardiac tamponade • Tension Pneumothorax • Mediastinal mass • Support ABC’s, but fluids may not be the best option. The obstruction must be relieved
Distributive Shock • Septic shock • Systemic infection as evidenced by a positive blood culture • Patient in early septic shock will have bounding pulses and warm extremities • Also known as warm shock
Distributive Shock • Septic shock: • Bacterial organisms release toxins, which results in an inflammatory response and cellular damage • Massive vasodilation-sometimes called “warm shock” • Increased capillary permeability • Fluid shifts to extracellular space • Hypotension may not respond to fluid resuscitation • Inotropic support • 80% of children in septic shock will require intubation and mechanical ventilation within 24 hours of admission
Distributive Shock • Neurogenic shock: • Severe head or spinal injury • Decreased sympathetic output from the CNS • Decreased vascular tone • Anaphylactic shock: • Antibody-antigen reaction stimulates histamine release • Histamine is a powerful vasodilator • Loss of vascular tone
Treatment of Shock • Early goal directed treatment improves outcomes • Needs to begin with the local emergency departments and continue with the transport team • Early aggressive interventions to reverse shock can increase survival by 9 fold if proper interventions are done early! • Hypotension and poor organ perfusion worsens outcomes • Shock can progress very quickly into refractory shock which is irreversible • Airway and Breathing • Have suction and airway adjuncts available • 100% O2 until more stable, then weaning can begin • Assess breathing effectiveness • If patient cannot protect their own airway, intubate! • Intubate for GSC of 8 or less!
Treatment of Shock • Circulation • Venous access: Ideally 2 large bore IV’s • Fluid resuscitation: 20ml/kg bolus of NS or LR • Reassess patient after each bolus • Convert to blood bolus if patient is bleeding • Saline cannot carry oxygen • Inotropic support for hypotension that persists despite fluid resuscitation-Beware of catecholamine resistant shock! • Treat hypothermia • Correct F/E imbalances • Find the cause and fix it! • Dextrose • Treat hypoglycemia and monitor closely
Case Study • 8 week old infant s/p cardiac arrest at home • Paramedics initiated CPR and continued CPR for 10 minutes until arrival in ED
Phone call • Patient arrived in ED with CPR in progress • Intubated with 3.0 ETT and being bagged • Epinephrine given X 2 • Atropine given X 2 • Heart rate resumed • Sodium Bicarb given X 2 • Vent settings: FiO2 1.0, Rate 40, PIP 20 PEEP 3 • Pupils 3mm and sluggish • Cap refill 5 seconds
Case Study-On arrival • Current vitals: HR-140 RR-40 BP-52/11 Temp- 90F • Vent settings: FiO2 1.0, Rate 40, PIP 20 PEEP 3 • Cap refill 5 seconds • ABG 6.93/74.4/259/14.8/-16.9 • 2 tibial IO’s in place bilaterally and one PIV with maintanance and dopamine infusing at 5 mcg/kg/min • Glucose-47, K-7.0 non-hemolyzed • Succinylcholine given by ED staff but patient with gasping respiratory effort
Case Study-Interventions • Re-tape and pull back ETT 1 cm • Increase PEEP to +5 • Sedation with Fentanyl 1-2 mcg/kg • Treat hypoglycemia-2ml/kg of D10W • Provide adequate paralysis with pavulon • Give Calcium Chloride-Why? • Give dextrose to increase accucheck to 100, then give regular insulin 0.1u/kg-Why?
Case Study-What happened? • Patient sedated and paralyzed appropriately • CaCl and bicarb given as ordered • Recheck of accucheck after dextrose =112 • Insulin given as ordered • Accucheck dropped to 42 so D10W repeated • One IO was infiltrated so new PIV started • Repeat ABG 6.94/92.1/233/18.8/-13.1 • BP dropped after pavulon, so dopamine titrated up-to 20mcg/kg/min • Pt diagnosed with Influenza