Download
1 / 23
250 likes | 707 Vues
Benign Joint Hypermobility Syndrome . Primary Care Conference November 28, 2007 Rebecca L Byers. Clinical Case. Patient: 45 yo woman with 2 ½ month history of right toe pain and one month of bilateral sciatica, with R>L.

E N D
Benign Joint Hypermobility Syndrome Primary Care Conference November 28, 2007 Rebecca L Byers
Clinical Case • Patient: 45 yo woman with 2 ½ month history of right toe pain and one month of bilateral sciatica, with R>L. • Hit toe against furniture in late August. Seen in UC and diagnosed with sprain. Wore a padded boot for several weeks with decrease in symptoms. Symptoms returned with regular shoe use.
Second visit – films of right toe showed tiny fragment dorsal to first MTP joint. No other abnormalities. • Third visit – now has bilateral pain radiating down both legs. L/S films show mild DDD L4-L5, L5-S1 and 18 degrees of convex-right scoliosis. Repeat toe films – absence of prior fragment, dx of hallux valgus.
Exam: Easily places palms on the floor. No vertebral tenderness, no SI joint tenderness. Negative SLRs – hyperflexible bilaterally (120 deg). Tenderness over right first MTP, not red, no swelling.
Past Medical History • Migraine headaches • MVA 1997 with headache and neck pain; resolved. Head CT negative. MRI neck with small C6 bulging disk without nerve root or spinal cord contact. • Right breast cancer 2001, positive sentinel node, 6/6 other nodes negative. Chemo x4 (adriamycin, cytoxan). Bilateral mastectomy with reconstruction/implants.
Joint Hypermobility-ability to painlessly perform one of the following maneuvers: • 1. Extend the 5th metacarpophalangeal joint more than 90 degrees, oppose the thumb to the forearm (picture 1).
2. Extend the elbow more than 10 degrees beyond neutral (picture 2)
3. Extend the knee more than 10 degrees beyond vertical (picture 3).
4. Place both palms on the floor without bending the knees (picture 4).
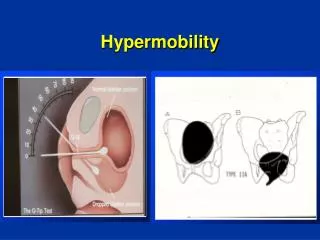
Beighton score Specific joint laxity Thumb to forearm, hyperextension of fingers, hyperextension of elbow or knee, palms to floor… Left, Right, Back Nine anatomic sites. Calculation if one point each with 9 being highest possible total.
Hypermobility Joint Syndrome • Disorder in which musculoskeletal pain and generalized joint hypermobility occur together. • The term benign hypermobile joint syndrome (BHJS) is used to distinguish this non-life threatening disorder from diseases such as the Marfan syndrome.
Diagnostic criteria for BJHS Major Criteria • 1. Beighton score of 4/9 or greater • 2. Arthralgia for more than 3 months in 4 or more joints. Minor Criteria • 1. A Beighton score of 1, 2 or 3/9 (0 to 3 if over age 50). • 2. Arthralgia for 3 months or more in 1-3 joints, or back pain for 3 months or more, of spondylosis, spondylolysis, or spondylolisthesis. • 3. Dislocation or subluxation in more than one joint, or in one joint on more than one occasion.
4. Soft tissue rheumatism in 3 or more locations (eg, epicondylitis, tenosynovitis, bursitis) • 5. Marfanoid habitus. • 6. Abnormal skin (eg, striae, hyperextensible, thin or papyraceous scarring). • 7. Eye abnormalities (eg, drooping eyelids, myopia, anti mongoloid slant). • 8. Varicose veins or hernia or uterine/rectal prolapse.
Pathogenesis • Thought to be a disorder of collagen that contributes to a loss of tensile strength, with increased fragility of the joint capsule, ligaments and tendons. • High concordance in female monozygotic twins (60%).
Prevalence • Generalized joint hypermobility – varies from 10 to 30%. More common in the right limb, females, blacks. Decreases with age. • BHJS – prevalence is less certain. Most studies done in Rheumatology clinics with rates similar to Rheumatoid Arthritis (i.e., about 1% of the population).
Clinical Manifestations • Wide range of musculoskeletal complaints -- brief joint “swelling”, symmetrical joint pain during use and relieved with rest, and arthralgias and myalgias without any apparent abnormality. -- back pain frequent; more common in women: one study showed that 17 of 20 women without another cause of back pain had joint laxity.
Other Possible Associated Symptoms • Anxiety/Panic Attacks • Cognitive Disorders • Palpitations • Shortness of breath • Fatigue • Orthostatic symptoms Postulation of disordered autonomic nervous system function due to chronic pain.
References • Beighton, PB, Grahame, R, Bird, HA. Hypermobility of joints, 2nd ed, Springer, New York 1989. • Bridges, AJ, Smith, E, Reid, J. Joint hypermobility in adults referred to rheumatology clinics. Ann Rheum Dis 1992; 51:793. • Gazit, Y, Nahir, AM, Grahame, R, Jacob, G. Dysautonomia in the joint hypermobility syndrome. Am J Med 2003; 115:33.
Graham, R, Bird, HA, Child, A, et al. J Rheumatol 2000; 27:1777. • Hakim, AJ, Cherkas, LF, Grahame, R, et al. The genetic epidemiology of joint hypermobility: a population study of female twins. Arthritis Rheum 2004; 50:2640. • Sheon, RP, Moskowitz, RW, Goldberg, VM. Soft Tissue Rheumatic Pain: Recognition, Management, Prevention, 3rd ed, Williams & Wilkins, Baltimore 1996.