Download

1 / 27
420 likes | 1.73k Vues
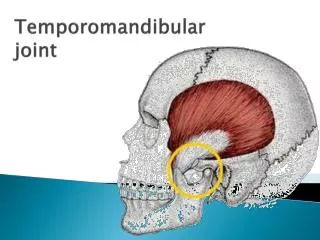
Temporomandibular Joint Disorder Syndrome (“TMJ”). MLK Med-Peds Laura Hanson, MS2. Definition of TMJ. Chronic or acute musculoskeletal pain with dysfunction of the masticatory system Distinct from dental disease Due in part to persistent, unconscious, repetitive use of masticatory muscles.

E N D
Temporomandibular Joint Disorder Syndrome (“TMJ”) MLK Med-Peds Laura Hanson, MS2
Definition of TMJ • Chronic or acute musculoskeletal pain with dysfunction of the masticatory system • Distinct from dental disease • Due in part to persistent, unconscious, repetitive use of masticatory muscles
Why is it hard to recognize TMJ? • Difficult to classify • Many overlapping syndromes, all based on symptomatology rather than etiology • Difficult to study a natural course or etiology • Large percent of general population has classic symptoms. (75% in one study) • Disease vs non-disease. • Physicians aren’t taught it- dentists are.
Why is it important to recognize TMJ? • Pain is the most common reason people seek medical attention • $80 billion each year in lost workdays, worker’s comp/disability, and healthcare • The prevalence of TMJ-related pain in 2000 was 12% (~2% will seek treatment), and 10 million Americans will suffer TMJ related complaints each year.
Types of TMJ • Intracapsular • Rheumatoid Arthritis • Articular disk displacement • Extracapsular • Myofascial/myogenic • More common
Stress Malocclusion Bruxism Clenching DJD Female Gender Cervical traction Dental manipulation Trauma Internal joint derangement Causes
Jaw Malocclusion • Very common • May be inherited or acquired • Braces, crowed teeth, extra teeth, missing teeth • May be a cause OR result of chronic masticatory muscle tension
Bruxism • Grinding • Control: 360 tooth contacts a night • TMJ: 1325 tooth contacts a night
Disk Displacement • Displacement may be anterior, lateral, or medial, and is NOT diagnostic • Study using MRIs • 84% of subjects with TMJ • 33% of asymptomatic subjects • Cadaver study • 40-60% incidence of displacement • No convincing evidence of progression to locking or joint degeneration.
Presenting Symptoms • Pain in muscles of mastication • Pain in ipsilateral ear, jaw, neck • Dull headache worsened with chewing • Sometimes only symptom is headache • Symptoms relate to stress • Audible clicking, crepitus, or locking (usually a sign of disc displacement)
Headaches • International Headache Society • http://www.i-h-s.org Guidelines ICHD-II Classification (pdf) • Primary Headaches • Migraine • Tension-Type Headache • Cluster Headache
Headaches cont’d • Secondary Headaches- Headache due to: • Head/Neck trauma • Vascular disorders • Non-vascular intracranial disorders • Substance use or withdrawal • Infection • Disorders of homeostasis • Disorders of cranium, neck, eyes, ears, nose, sinuses, teeth, mouth, or other facial/cranial structures • Psychiatric disorders
Headache attributed to TMJ • Recurrent pain in one or more regions of the head and/or face, + C and D • Xray, MRI, and/or bone scintigraphy demonstrate TMJ • Evidence that pain is related to TMJ: (at least 1) • Movement and/or chewing • Decreased range of motion or irregular jaw opening • Noise from one or both joints during movement • Tenderness of one or both joint capsules • Headache resolves within 3 months, and doesn’t recur, after successful treatment of TMJ
Physical Exam • Inspection: • Body or facial asymmetry • Deviated jaw motion • Restricted or guarded jaw motion • Should NOT see swelling • Also observe for crepitus/clicking
Physical Exam • Palpation • Palpate the joint intra/extraorally with mouth open and closed to find tenderness • Palpate the masseter over the angle of the jaw bilaterally • Palpate the temporalis over a wide area, both clenched and relaxed • Palpate the pterygoid inside the mouth • Note any clicking/crepitus
Radiology • Limited yield • Panorex, Periapical radiographs, CT - evaluate bony structures for DJD or disc displacement (no change in outcome) • MRI will show the disc • Consider imaging when dental problems are suspected or if conservative management fails (evaluating for surgery).
Prognosis • Rule of thirds: 235 patients studied with TMJ • 33% resolved • 31% ongoing pain • 36% relapsing course
What should you do? A 37 year old female in law school presents to your office with the chief complaint of headache. It is frontal and bitemporal, and is associated with photophobia, but no nausea. You prescribe migraine medication, but she returns in one week with persistent headache. What now?
Not a migraine, huh… • What symptoms do you want to ask about? • What will you look for on physical exam?
Management • Support • Education • Exercise, massage • Acrylic appliance • Pain Relief (NSAIDs, TCAs,muscle relaxants, narcotics) • Injections • Surgery
Sources • Sheon, Robert P. “Temporomandibular Joint Dysfunction Syndrome”. UpToDate, June 2005. • Gremillion, Henry A. “The Prevalence and Etiology of Temporomandibular Disorders and Orofacial Pain”. Texas Dental Journal, July 2000. • DeBont, Lambert GM., et al. “Epidemiology and natural progression of articular temporomandibular disorders”. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 1997.