Download
1 / 31
310 likes | 381 Vues
Learn about von Willebrand disease and sickle cell disease, their clinical manifestations, treatments, and impact on disability determination. Includes Sickle Cell Trait risks and management of vaso-occlusive crisis.

E N D
Heme Update for Disability Determination(vonWillebrand and Sickle cell) Jennifer M Pearce MD September 2010
vonWillebrand Disease What is it? --vW protein important for start of clot—attracts platelets and helps them stick to bleeding site --Type I vW disease is most common—make the protein but have reduced (not absent) quantities making clotting difficult --Type II vW—make an abnormally functioning protein --Type III vW—no protein made and have severe bleeding
Clinical Manifestations of vW In general bleeding is not severe enough to cause disability Don’t have joint bleeds or spontaneous bleeding Primarily mucosal bleeding --nosebleeds --gum bleeding/dental work --bleeding with tonsillectomy etc Menorrhagia --can be incapacitating but that is rare --can cause significant iron deficiency
Treatment of vW Use of DDAVP as IV or intranasal to raise vW levels Use of antifibrinolytics Infusion of blood derived vW protein Hormonal control of menses
Is vW a reason for Disability? • Essentially NO unless there are unusual extenuating circumstances
Sickle Cell Disease With all the variants affects 1:600 African Americans, 1:12 are carriers Can also occur in other ethnic groups: India, Italy, Spain, Saudi Arabia, Greece Variants: SS, SC, S-Beta Thal, SD --but in all S is the primary hemoglobin --SS have, in general, more problems
Lifespan in Sickle Cell Used to be quoted in 20s because of overwhelming infectious deaths in early childhood Now in 40s and death is usually from endstage heart, kidney or lung disease or hemorrhagic stroke
Sickle Cell Trait One Beta chain has sickle and the other is normal 8% of African-Americans, 0.5% Hispanics, 0.2% Caucasians in United States Only sickle in extreme circumstances Increased risk exertional rhabdomyolysis, spenic infarction and renal medullary carcinoma 10-30x increase of exercise induced death—recent NCAA ruling Generally have no symptoms or issues except in extreme and avoidable situations
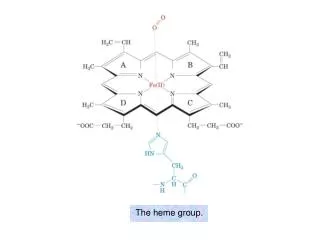
Hemoglobin • Normal is 2 alpha chains and 2 beta chains floating in red cell as a foursome—they don’t stick to another foursome • In Sickle cell the beta chains have a mutation that, when the hemoglobin unloads oxygen normally, allows the tetramers to stack together in a polymer
The red cell • Red cells unload their oxygen in the capillaries • Capillary diameters are smaller than a red cell • When sickle cells deoxygenate their shapes change and if they are still in the capillaries they get stuck
Vaso-occlusive crisis Essentially deep pain from tissue death in the region where blood flow occluded Often extremities but can be anywhere Precipitated by anything that slows blood flow through the capillaries or increases rate of deoxygenation Can happen any time and can last from hours to days—episodic, unpredictable, last from a day to a week Prolonged pain often requires narcotics Addiction rare, respiratory depression rare
What leads to a crisis? • Anything that leaves the pliant red cell in the capillary long enough to undergo shape change and get stuck • Causes oxygen to unload more quickly (increased tissue demand, acidosis) • Slows blood flow (cold, vessel constriction, dehydration)
Factors that precipitate a crisis Physical Cold—a few degrees of change, warmth of clothing, heat in house, swimming Hypoxia—high altitudes, asthma, sleep apnea Acidosis—don’t go for the “burn” Dehydration—and kidneys can’t concentrate Weather changes Another illness—URI etc Hormonal—menstrual cycle
Treatment of a crisis Pain relief and anti-inflammatories Start with Tylenol and Ibuprofen, then codeine and on up to morphine/narcotic Hydration—oral or intravenous Heat Rest Correct inciting factors
Other Issues=Anemia Stiff damaged cells are removed rapidly from circulation --normal non sickle red cell lives 120 days --normal sickle cell lives 20 days Marrow can’t keep up so usually hemoglobin is 6.5-9gm/dl instead of >10 impacts growth and development: increased caloric needs of marrow “machine”
Other Issues=Overwhelming sepsis • Primarily in the younger child; starts at 4 months of age --15% incidence without penicillin prophy --30-50% mortality (2/3 of deaths within 8 hours) • Mostly from ineffective spleen which is gradually “killed off” by sickling • Try to prevent with vaccines and prophylactic penicillin • Rapid intervention with fevers
Other Issues=Stroke • 10% of kids, peak age for ischemic=7 • Older adolescents/young adults: hemorrhagic stroke=50% fatal • 2/3 incidence of recurrence unless transfused • Screen with TCD and MRI/MRA • Stroke --Often silent --Thrombotic in kids, hemorrhagic in adults --?reason for learning problems in kids --mandates transfusions/bone marrow transplant
Other Issues=Cardiac • Pump wears out faster: cardiomegaly and LVH • Pulmonary hypertension, cor pulmonale • Iron overload with cardiomyopathy
Other Issues=Acute chest • Pneumonia vs vaso-occlusive crisis in chest • Or a bit of both • Rapid progression of symptoms • Major cause of death
Other issues=Chronic lung disease • Concurrent asthma • Progress to pulmonary fibrosis • Pulmonary arterial hypertension (PAH) • Puts additional stress on heart, pumping against higher pressure • 30% of adults who were screened • 75% on autopsy • 40-50% 2 year mortality when severe PAH
Renal • Inability to concentrate urine • Happens early in life • Become dehydrated more easily • Hematuria/proteinuria • Nephrotic syndrome • Renal failure
Avascular necrosis • SC and SS • “death” of femoral/humeral head • Pain and disability
Other Issues=Vision • Develop retinopathy as age (starts in teens) • Can seriously affect vision
Other Issues=miscellaneous Aplastic crisis Gallbladder disease Skin ulcers: poor healing Splenic sequestration In 5-24 mo of age, rapid onset with severe anemia Life threatening
Lifestyle in Sickle Cell Uncertainty always about tomorrow --makes education and employment tough --average 24 days/year in the hospital --many days at home unable to work or be in school --parents lose work days Some patients more affected clinically than others—why? Social stigma re narcotic use even if very appropriate
Sickle Cell “Cure” Bone Marrow Transplant --difficulties with finding donors --post transplant complications --New group of disabling/chronic conditions Gene therapy--?? the future
Sickle cell treatment • Chronic transfusion therapy --iron overload --red cell sensitization • Hydroxyurea—can be wonder drug • Increases fetal hemoglobin levels which interfere with sickling • Improves anemia, decreases organ damage, decreases incidence/severity of VOC