Download
1 / 66
680 likes | 994 Vues
Rick Stouffer MD University of North Carolina. Renal Artery Stenosis – The Good, The Bad and The Different. Disclosure. I will discuss off-label uses No financial conflicts of interest. The ‘classic’ patient for renal artery revascularization. 55 year old male HTN, known CAD (prior PCI)

E N D
Rick Stouffer MD University of North Carolina Renal Artery Stenosis – The Good, The Bad and The Different
Disclosure I will discuss off-label uses No financial conflicts of interest
The ‘classic’ patient for renal artery revascularization • 55 year old male • HTN, known CAD (prior PCI) • Admitted with CP/SOB, BP 194/124 mm Hg • BP Rx: ACEI, beta blocker, nitrate • Creatinine 1.6 mg/dl, HCT 41.8% • Referred for cardiac catheterization
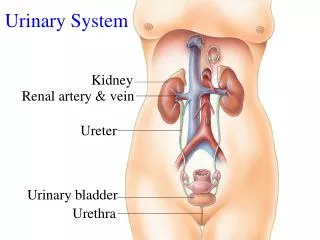
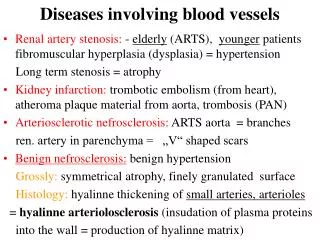
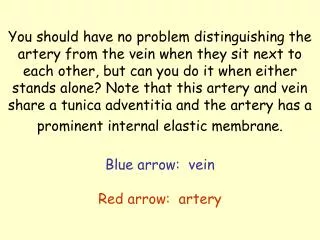
Renal angiography + hemodynamic assessment Aorta Right renal artery
Accelerated HTN Mild elevation in creatinine Symptoms Renal artery revascularization
Outline • Types of RAS • Atherosclerotic RAS • Natural history of the patient with RAS • Treatment of RAS
Renal Artery Stenosis • Atherosclerotic (90%) • Fibromuscular dysplasia (10%) • Medial fibroplasia (90%) • classic "string of beads" appearance • middle-to-distal portion of the artery • Perimedial fibroplasia • focal stenoses • Intimal/Medial fibroplasia • a focal, concentric stenosis • Aortorenal dissection • Vasculitis involving the renal artery (i.e. PAN) • AVMs involving the renal artery • Irradiation of the renal artery • Scleroderma
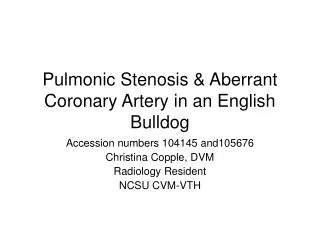
FMD – Anatomy and Pathophysiology 70 year old female with chest pain and 4-drug hypertension. Circulation. 2005;112:e278-9.
Before balloon angioplasty After balloon angioplasty
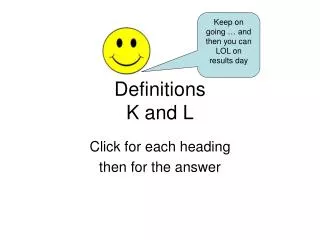
A Cautionary Tale • 37-year-old male admitted with headache of six months duration that had worsened in the last week and was accompanied by blurry vision, dyspnea on exertion and weakness in his legs. • No significant PMH, was not taking any medications and had never been diagnosed with hypertension. No history of alcohol or drug use. • FH - mother with hypertension and a sister with migraine headaches. • Brachial BP was 252/160 mm Hg with no significant difference between arms.
A Cautionary Tale • BP = 252/160 mm Hg • Ophthamology consultant - Grade IV retinopathy including marked AV nicking and venous dilatation, cotton wool spots, large areas of choroidal ischemia, delayed vascular filling, blind spots and papilledema in both eyes. • MRI of the brain - No evidence of intracerebral mass but increased signal abnormality within the pons, consistent with hypertensive encephalopathy. • MRI/MRA of the abdomen showed normal kidney size, no renal or adrenal masses and ‘No evidence of renal artery stenosis.’
FMD not visualized on MRI/MRA Balloon angioplasty with resolution of pressure gradient J Invasive Cardiol. 2007;19:E31-3.
5 years later - He has run marathons and climbed Mount Kilimanjaro. Home systolic BPs of 130 mm Hg on HCTZ 20 mg daily, enalapril 10 mg daily and Norvasc 10 mg twice daily.
Outline • Types of RAS • Atherosclerotic RAS • Natural history of the patient with RAS • Treatment of RAS
Usually ostial Associated with diseased aorta Can be unilateral or bilateral Atherosclerotic RAS
Prevalence of Atherosclerotic RAS • 6.8% in healthy adults > 65 years old • Evaluation with renal artery duplex of 834 patients consecutive patients who were participants in the Forsyth county cohort of the Cardiovascular Health Study (J Vasc Surg. 2002;36:443–51). • Unselected autopsies 4-27% • Hypertensives 1-4% • Aged 65 years and older 6.8% • Diabetics 8%
RAS is common in patients with vascular disease • Prevalence of RAS • Proven MI 12% • Undergoing cardiac catheterization 6-19% • Lower extremity PVD 22-59% • Predictors of RAS in patients undergoing cardiac catheterization • CAD; Age; PVD; serum creatinine; hypertension
Severe HTN Physiologic testing for RAS Renal Angio (anatomic) Revascularization Traditional Paradigm of Renal Artery Stenosis
Chest pain, dyspnea, etc Evaluation for Vascular Disease (usually CAD) Severe HTN Physiologic testing for RAS Renal Angio (anatomic) Revascularization The Changing Paradigm of Renal Artery Stenosis
Outline • Types of RAS • Atherosclerotic RAS - Prevalence and 'Risk factors' • Natural history of the patient with RAS • Treatment of RAS
Dismal Prognosis Associated with RAS 3 year mortality 26% in patients treated with stents (Circulation 1998;98:642-647) 28% in patients managed medically (Mayo Clin Proc 2000;75:437) 4 year mortality 43% in patients with RAS discovered incidentally at cardiac catheterization (Kidney International 2001;60:1490-1497) 35% in patients with RAS discovered incidentally at cardiac catheterization (JASN 1998;9:252-256) 26% in a multi-center study of patients undergoing percutaneous renal revascularization (Circulation 1998;98:642-647) 5 year mortality 33% in a single-center study of patients undergoing percutaneous renal artery revascularization (Catheter Cardiovasc Interv. 2007;69:1037)
Effect of RAS on Prognosis – Relative Five year Survival Ries LAG et al. SEER Cancer Statistics Review, 1973-1998. National Cancer Institute. September 2000.
Clinical Events in Patients With RAS Claims data from a 5% random sample of the United States Medicare population were used to select patients without atherosclerotic renovascular disease in the 2 years preceding December 31, 1999 (N= 1,085,250), followed until December 31, 2001. J Am Coll Cardiol Intv 2009;2:175-182
The $64000 Question Is RAS a marker of severe atherosclerosis and thus portends a poor prognosis? or Does RAS contribute to progression of vascular disease - thus implying that effective treatment may improve clinical outcomes?
Outline • Types of RAS • Atherosclerotic RAS • Natural history of the patient with RAS • Treatment of RAS
Optimal Medical Treatment • ARB + diuretic to get BP to target • <140/90 mm Hg • <130/80 mm Hg with DM • LDL to goal • Currently <100 (or 70) mg/dl • Diabetes Management • HbA1c to target (<7%) • Smoking Cessation • Anti-platelet therapy (aspirin +/- clopidogrel/prasugrel)
Percutaneous Treatment of RAS 1978 - Gruentzig and colleagues report first balloon angioplasty of renal artery stenosis Gruentzig A, Kuhlmann U, Vetter W. Treatment of renovascular hypertension with percutaneous transluminal dilatation of a renal artery stenosis. Lancet 1978; 1:801-802. Fall 1978 - first renal artery angioplasty in US at UVa. - Patient referred by Carlos Ayers to Charles Tegtmeyer who obtained angioplasty balloon from Gruentzig in exchange for fishing equipment. Tegtmeyer CJ, Dyer R, Teates CD, Ayers CR, Carey RM, Wellons HA Jr, Stanton LW. Percutaneous transluminal dilatation of the renal arteries: techniques and results. Radiology 1980; 135(3);589-599
Evidence-based Medicine • Reviewed 55 studies • “Almost two thirds of the studies that we reviewed were of poor methodologic quality; none was deemed to be of good quality.” • “More than half of the studies had limited applicability to patients commonly seen in practice or to modern management strategies.” • “No study directly compared angioplasty with stent placement and "aggressive" medical treatment with currently available antihypertensive, antiplatelet, and lipid-lowering agents.”
Effect of RA Revascularization on HTN Study Device N Cure Improved Klinge stent 134 10% 68% Lossino stent 153 12% 51% DRASTIC balloon 106 7% 68% Rocha stent 150 6% 50% Dorros stent 145 1% 52%
Effects of RA Revascularization on Ischemic Nephropathy Prog Cardiovasc Dis 2007;50:136
Angioplasty and STent for Renal Artery Lesions NEJM 2009;361:1953-1962
ASTRAL Trial No revascularisation (n = 403) Medical treatment according to local protocol Revascularisation (n = 403) with angioplasty and/or stent (and medical treatment) Substantial atherosclerotic RAS Suitable for endovascular revascularization Patient's doctor was uncertain that the patient would benefit from revascularization
Procedural Complications • 38 periprocedural complications in 31 of the 359 patients (9%) who underwent revascularization (including 1 of the 24 patients in the medical-therapy group who crossed over to revascularization) • Nineteen of these events (in 17 patients) were considered to be serious complications • Pulmonary edema (1) and Myocardial infarction (1) • Renal embolizations (5), Renal arterial occlusions (4) and Renal-artery perforations (4) • Femoral-artery aneurysm (1) • Cholesterol embolism leading to peripheral gangrene and amputation of toes or limbs (3)
“An important limitation of our trial concerns the population that we studied. As noted, patients were enrolled in the trial only if their own physician was uncertain as to whether revascularization would provide a worthwhile clinical benefit.” • Patient selection (single center) • 508 patients with atherosclerotic renovascular disease • Of these, 283 patients had renal-artery stenosis of more than 60% • 71 underwent randomization • 24 underwent revascularization outside the trial • poorly controlled hypertension • rapidly declining renal function, • 188 received medical treatment only.
Criticisms of ASTRAL 1. Selection bias and inexperienced operators • ‘On average, 2 patients per center per year underwent randomization, which indicates serious selection bias or inexperienced staff at centers with very low intervention rates. This concern is supported by a low rate of technical success (317 of 403 patients [79%] in the revascularization group) and a high rate of serious complication in 23 of 280 patients (8%) as compared with reports in the literature of 98% and 2%, respectively.’ NEJM 2010;362:762
Criticisms of ASTRAL 2. There was a reduction in the number of antihypertensive drugs in stent treated patients • ‘The study design implies that optimal medical therapy was used to achieve normalized blood pressure in both groups. Thus, not only the blood pressure values but also the number of antihypertensive drugs used to achieve this goal should be taken into account. The … significantly lower number of antihypertensive drugs administered in the revascularization group (P=0.03) preclude the definitive conclusion that renal-artery revascularization provides no clinical benefit.’ NEJM 2010;362:762