Download
1 / 39
2.12k likes | 5.61k Vues
ROLE OF NUTRITION IN ICU PATIENTS. PRESENTED BY-DR.NITIN SHANKER MODERATER-DR.V.MURALIDHAR . www.anaesthesia.co.in anaesthesia.co.in@gmail.com. AIMS OF NUTRITIONAL SUPPORT. Provide exogenous substrates to meet micro and macro nutrient requirement in ICU patients.

E N D
ROLE OF NUTRITION IN ICU PATIENTS PRESENTED BY-DR.NITIN SHANKER MODERATER-DR.V.MURALIDHAR www.anaesthesia.co.inanaesthesia.co.in@gmail.com
AIMS OF NUTRITIONAL SUPPORT • Provide exogenous substrates to meet micro and macro nutrient requirement in ICU patients. • Help protect vital visceral organs and attentuate breakdown of skeletal muscle. • Reduce net protein catabolism.
FACTORS ASSOCIATED WITH MALNOURISHMENT • Chronic diseases like malignancy,kidney and liver diseases,Congestive heart failure. • Digestive and absorptive abnormalities like inflammatory bowel disease,short bowel syndrome,gastrointestinalfistula,pancreaticdisease,chronicdiarrohoea. • Social and dietary factors.i.e.Drug and alcohol abuse,poverty and poor dentation. • Increased requirements as in burns,post-surgery, sepsis and chemotherapy patients. • Critically ill patients and mechanically ventilated patients.
EFFECTS OF MALNUTRITION IN ICU OUTCOME: • Impaired immunological function. • Impaired ventilatory drive. • Prolonged ventilator dependence. • Increased infectious mortality and morbidity. • Increased risk of complications. • Poor wound healing. • Increased length of ICU stay.
ESPEN CRITERIA FOR SEVERE UNDERNUTRITION: Atleast one of the criteria should be present: • Subjective Global assessment Grade C.(evaluates abnormalities in food intake,digestion an absorption,strength and activity,and body composition). Developed by Detsky et al.Goodsenstivity and specificity. • Serum albumin level <30gm/litre(with no evidence of hepatic or renal dysfunction. • Weight loss of 10%-15% in period of 6 months.
NUTRITION AS A SOURCE OF ENERGY Basal Energy Expenditure (BEE) or BMR-The energy expenditure on awakening from a 12 hour fast measured in a thermoneutral environment(25 deg). Thermogenic Effect of Food(Specific Dynamic Action)-The energy exenditure after the ingestion of food.Increases by 5%-10% Sleeping Energy Expenditure-During sleep.Usually 10%-15% lower than REE.
Resting Energy Expenditure(REE)-Energy expenditure while resting in supine position with eyes open.Includes the thermogenic effects of food if performed within hours of a meal or during continous infusions of nutrients such as during TPN administration.10% greater than BEE. Activity Energy Expenditure(AEE)-During maximum exercise 6-10 fod greater than BEE. • Fever increases metabolic rate by 10% per degree centigrade rise in temperature.
Estimating Resting Energy Expenditure(Harris-Benedict Equation)- Male eBEE(Kcal/day)=66+(13.7.W)+(5.H)-(6.8.A) Female eBEE(Kcal/day)=655+(9.6.W)+(1.7.H)-(4.7.A) eREE=eBEE.Stress factor eTEE=eREE.Activity factor
Measuring Energy Expenditure using Indirect Calorimetry Weir Equation=1.44(3.9.VO2)+(1.1VCO2) Measured with help of specialized instruments known as metabolic carts. Recommended method of measurement in critically ill patient* Limitations- • Expensive equipment • Patient should be on ventilator • Oxygen sensor unreliable at inspired levels above 50% * Flancbaum et al.Comparison of indirect calorimetry,theFick method and prediction equationsin estimating the energy requirements of critically ill patients AJC Nutrition;1999;69:461-466
Nitrogen Balance(as a measure of protein requirement)- • Two thirds of nitrogen derived from protein breakdown is excreted in urine. • Protein is 16%nitrogen-each gram of urinary nitrogen (UN) represents 6.25 gms of degraded protein. N Balance(gm)=(Protein intake(gm)/6.25)-(UUN+4) UUN=Urea Nitrogen excretion(gm) in 24 hrs • The first step in achieving a positive nitrogen balance is to provide enough non protein calories to spare proteins from being degraded.
Calories can be provided in three forms- Carbohydrates- • Provide 30%-70% of total calories. • Commonly in form of glucose but sucrose,fructose are also used. • Insulin maybe required to maintain tight sugar control(since Insulin resistance is seen in stress). Fat- • 20%-50% of total calories. • Critically ill patients utilize fat better than carbohydrates as energy source. • Atleast 7% of total calories should be in form of omega-6-polyunsaturated fatty acid(PUFA) triglycerides. • Medium and long chain triglycerides.
Proteins- • 15%-20% total calories to be given as proteins.Administered as whole proteins or amino acids.
Stress factors- Spontaneously breathing non-sedated patients: • Major surgery 15%-25% • Infection 20% • Long Bone fracture 20%-35% • Malnutrition subtract 10%-15% • Burns upto 120% depending upon extent • Sepsis 30%-55% • Major Trauma 20%-35% • COPD 10%-15% • Sedated mechanically ventilated patient subtract 10%-15%
Activity factors • Sedated mechanically ventilated patients 0.5% • Bedridden spontaneously breeathing non sedated patients 10%-15%. • Sitting in chair 15%-20% • Ambulating patients 20%-25%
ASSESSMENT OF NUTRITIONAL STATUS IN CRITICALLY ILL PATIENTS • Body Mass Index (Anthropometric measure) • Skinfold thickness and arm-muscle circumference. • Creatinine height index • Temporal wasting • Signs of specific micronutrient deficiency. • Albumin-protein nutritional status • Prealbumin levels are a better indicator nutritional status. • Hemoglobin levels • Magnesium • Phosphorus
CUTHBERTSON MODEL OF RESPONSE TO INJURY: • Ebb phase-Period of severe shock,depression of enzymatic activity and oxygen consumption. Reduced cardiac output and presence of lactic acidosis. • Flow catabolic phase-Fat and protein mobilization,increased urinary nitrogen excretion and weight loss. • Flow anabolic phase-Restoration of fat and protein stores and weight gain.
HIGHER METABOLIC REQUIREMENTS: • Burns • Septic Shock • Perfusion deficit • Inflammation • Necrotic tissues • Head Injury and polytrauma
CALCULATION OF ENERGY REQUIREMENTS: • As per ESPEN guidelines 2006 Acute initial phase of critical illness 20-25 kcal/kg/day Recovery/anabolic phase 25-30 kcal/kg/day
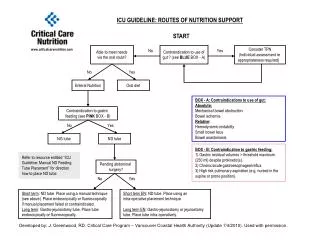
METHODS OF NUTRITIONAL SUPPORT Enteral feeds • Gastric feeds • Duodenal feeds • Jejunostomy feeds Total parenteral nutrition • Peripheral route • Central route
FORMULAS FOR FEEDING Carbohydrates • EN:Oligo- and polysaccharides • PN:Concentrated glucose Lipid • EN:Long and medium chain triglycerides • PN:soya bean oil,glycerol,eggphosphatides Nitrogen • EN:intact proteins • PN:Crystalline amino acid solutions Water and electrolytes Micronutrients
INDICATIONS FOR ENTERAL NUTRITION • Malnourished patients whose oral intake is poor for 3-5 days. • Well nourished patients with poor oral intake for 7-10 days.Inadequately for whatever reason to eat adequately. • Following massive bowel resection-enteral nutrition helps in regenaration of small bowel mucosa. • Enterocutaneous fistulae with an output of <500 ml/day. • Severe full thickness burns-limits sepsis and reduces protein loss from bowels.
Following major upper GI surgery • Following surgery for necrotising,suppurative pancreatitis-intial TPN followed by jejunostomy feeds.
CLASSIFICATION OF ENTERAL FEEDS Liquidized or Blenderized Food-Liquid forms of table food. Lactose-free formulas-Patients with lactose intolerance eg.Isocal,Sustacal Chemically defined formulas-Hydrolysated protein to facilitate absorption.eg.criticare HN Elemental formulas-Contain aminoacids.Well absorbed in jejunum.
FEEDING FORMULAS • Caloric density of feeding formulas determined by carbohydrates.Normally 1-2kcal/litre. • Osmolality of liquid feeding formulas varies from 280-1100. • Contain 35-40 gm protein/per litre.High protein diet feeds also availaible. • Lipid content of most formulas restricted to 30% of total calories. • Other additives-Glutamine,dietaryfibres,Branched chain amino acids,carnitine
COMPLICATIONS OF ENTERAL FEEDING • Gastric retention,vomiting, and aspiration pneumonia. • Diarrhoea • Mechanical problems
INDICATIONS FOR PARENTRAL NUTRITION • Non functioning gut e.g.paralyticileus. • Malnourished patients in whom the use of intestine is not anticipated for > 7 days after major abdominal surgery • Severe mucositis following systemic chemotherapy, upper gastrointestinal strictures or fistulae and severe acute pancreatitis where jejunal feeding is contraindicated. • In patients with major resections of small intestine (short bowel syndrome) before compensatory adaptation occurs.
COMPLICATIONS OF PARENTRAL NUTRITION Metabolic complications- • Hyperglycemia or hypoglycemia • Hypomagnesaemia • Hypophosphataemia • Hepatic dysfunction Catheter related- • Catheter related sepsis • Thrombosis of vein Technical complications • Catheter related
NUTRITIONAL SUPPORT IN SPECIAL CONDITIONS RENAL FAILURE- • To be started along with hemodialysis/hemofiltration. • Non-dialysed patients protein intake restricted to 0.5g/kg/day.Fluid restriction-0.8-1 litre/day if low urine output. • Dialysed patient protein intake increased to 1g/kg/day. • Incase of enteral feeding carbohydrate:fat ratio 60:40 • During haemodialysis loss of 6-12g of amino acid per treatment & loss 25-30 gm during a 6 hour dialysis. • Haemofilration net loss of 4 gm aminoacids. • Peritoneal dialysis net gain in glucose of 120-150 gm/day.
Hepatic failure- • If no encaphalopathy then protein-1gm/kg/day.If present then 0.3 gm/kg/day. • Infusion of branched chain amino acids improves encaphalopathy. • Caloric requirement of Glucose and fat in ratio 60:40 • Total caloric requirement 25 kcal/kg/day.
Respiratory failure- • Reduce carbohydrate intake to decrease carbon dioxide production especially when being weaned from ventilatory support. • Carbohydrate:fat ratio 40:60;protein intake 1.2 gm/kg/day.Total caloric intake 25 kcal/kg/day. • On the contrary patients with ARDS,lipid emulsions may interfere with gas exchange.Keepcarbohydrate:fat ratio 65:35 when on parenteral nutrition.
Cardiac Failure- • Restrict water and salt intake with careful monitoring of Na,K and Mg • TPN to be started with half caloric requirement over 3-4 days in order to avoid pulmonary oedema secondary to refeeding and increased metabolic rate. • Glucose:fat ratio 60:40
Pancreatitis- • To start enteraljejunal feeds of peptide based diet unless patient having fulminant pancreatitis or in sepsis. • Caloric intake of 25 kcal/kg/day with 1-1.5 gm/kg/day of proteins.
Burns- • Total caloric intake 30-35 kcal/kg/day with 2-2.5 gm/kg/day of proteins. • Increased protein intake reduces morbidity and mortality. • Prefered route enteral;maybe supplemented with TPN.
Pharmaconutrition:An emerging paradigm • Specific nutrients found to have effects on immune system,metabolism and GI structure and functions. • Glutamine • Arginine • Omega 3 fatty acids • Anti-oxidants
ROLE OF IV GLUTAMINE WITH PARENTRAL NUTRITION • Important immunonutrient derived from muscle protein breakdown. • Increased consumption in catabolic states thereby leading to: • Increased translocation of bacteria or bacterial toxins. • Decreased activity of macrophages and killer cells in the intestinal wall. • Increased risk of sepsis. • Increased morbidity and mortality. • Prolonged ICU stay.
Canadian Guidelines on Nutritional Support 2009 • Strongly recommend enteral nutrition over parentral. • Enteral nutrition to be commenced early(within 24-48 hrs)in ICU patients unless contraindicated otherwise. • When starting enteral nutrition strategies to optomize delivery of nutrients(starting at target rate,higher threshold of residual gastric volumes,use of prokinetics and small bowel feedings)should be considered. • Not to use diet supplemented with Arginine • When starting enteral feeds make use of whole protein formulas.
Reduced chances of pneumonia associated with small bowel feeding as compared to gastric feeding. • Maintain tight blood sugar regime(as per NICE sugar study maintain between 7-9 mmol/litre). • Consider supplementation of vitamins and trace elements. • Role of Selenium and other anti-oxidants is doubtful.
thanks www.anaesthesia.co.inanaesthesia.co.in@gmail.com