Download
1 / 34
340 likes | 541 Vues
Increasing Screening and Interventions for Four Unhealthy Behaviors. Jim Mold, M.D., M.P.H. Dept. of Family and Preventive Medicine OUHSC, OKC. Jim Mold Cheryl Aspy Zsolt Nagykaldi Millisa Ellefson Eileen Merchen Cara Vaught Katy Smith. Mike Aaron Sharad Swami Tamara Hartsell

E N D
Increasing Screening and Interventions for Four Unhealthy Behaviors Jim Mold, M.D., M.P.H. Dept. of Family and Preventive Medicine OUHSC, OKC
Jim Mold Cheryl Aspy Zsolt Nagykaldi Millisa Ellefson Eileen Merchen Cara Vaught Katy Smith Mike Aaron Sharad Swami Tamara Hartsell Heather Tipsword Ingrid Jackson Suben Naidu Zack Bechtol Rene Russell Shawn Anderson Research Team
Funding Source The Robert Wood Johnson Foundation Project Period 7/1/2005 – 9/30/2007
Challenge • More than 50% of premature deaths in the U.S. are the result of one or more of the four unhealthy behaviors: unhealthy diet, inadequate exercise, use of tobacco, abuse of alcohol • Effective screening methods exist for all four and effective brief counseling strategies are available for tobacco and alcohol and possibly exercise • Primary care clinicians are not consistently screening for these behaviors or intervening when they are discovered.
Primary Research Question Will a multi-component translational strategy result in the consistent and sustainable delivery of effective screening, very brief interventions, and counseling for improving diet, increasing exercise, and reducing cigarette and alcohol use among patients 14 years old and older being seen in primary care practices. Research Question
Research Aims • Offer and provide the translational strategies - training, practice facilitation, quality circles, and peer support - to geographically clustered primary care practices, and determine rates of adoption, implementation, reach, and sustainability; • Estimate the cost of the translational intervention and the cost to the practices of implementation; and • In conjunction with other RWJF funded teams, estimate the effectiveness of systematic screening and behavioral interventions delivered in primary care settings.
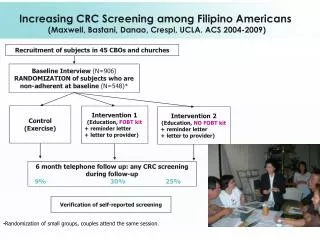
Practice Interventions Screening: Addition of evidence-based screening questions to the vital signs process Very Brief Interventions: Referral to a community-based resource or provision of written educational material Brief Counseling: 5 - 15 minute evidence-based counseling provided by the clinician
Translational Strategies Chart Audit and Feedback: Chart audits Q1month to document proportion of patients screened and proportion receiving interventions Training Modules: Three evidence-based training sessions (five modules) for clinicians and staff Practice Facilitation: Coordination of QI activities and assistance with obstacles (e.g. form/template redesign; identification of community resources, etc.) by PEA
Translational Strategies Quality Circles: Q2month lunch meetings during which geographical clusters of practices met to review progress, address problems, and share successes PI Visits: Q6month visits by PI during patient care activities to observe and ask questions about the processes, answer questions, and make suggestions.
Training Modules • Stages of change and motivational interviewing • Healthy eating and weight control • Exercise • Smoking cessation • Alcohol use reduction
Training Modules • Pretest • General Information • Evidence regarding effectiveness of screening and brief interventions • Role play scenarios • Post-test Training time was reimbursed and evidence-based (double) CME was awarded.
QI Process: PDSA Cycles PLAN: Small change proposed DO: Trial in a small number of patient encounters STUDY: Documentation of what happened ACT: Decision regarding what to do next (expand, abandon, modify)
Practice Facilitation (cont) • Identification of community resources • Weight loss programs • Alcohol counselor • Development of materials • Adolescent high-risk behaviors • Flow sheets and templates • Vital signs flow sheets • EHR templates • Wall charts
Design Interventions were introduced in 6-month cycles, each group of practices adding different interventions each cycle.
Data Collection • Practice Information Form (by practice facilitators) • Practice Assessment Template (by research assistant) • Knowledge Tests pre- and post-training (by clinicians and MA/nurse)
Data Collection Chart audits: 75 randomly-selected records; screening, VBI, BC at that visit Patient surveys (pre-office visit and 1-month later via mail): patients recruited/enrolled by practice facilitator in practices’ waiting rooms; f/u surveys mailed by project manager
Data Collection Practice facilitator diaries Field notes from quality circle meetings PI and Co-PI notes
0 1 2 3 4 5 6 PIF/PAT Field Notes Patient Surveys Training QC PI Visit QC Plan-Do-Study-Act Cycles Baseline Audit Audit PEA Audit PEA Audit PEA Audit PEA Audit PEA Audit
Participating Practices 1. W. Oklahoma (Clinton/Weatherford) • Mike Aaron, M.D. • Sharad Swami, M.D. • Tamara Hartsell, NP 2. Central Oklahoma (OKC) • Heather Tipsword, D.O. • Ingrid Jackson, M.D. • Suben Naidu, M.D. 3. E. Oklahoma (Grove) • Zack Bechtol, M.D. • Rene Russell, M.D. • Shawn Anderson, M.D.
Cost of the Intervention (Per 1000 patient encounters estimate) Screening (1000): $200 Very brief interventions (400): $ 80 Brief counseling (50): $830 TOTAL: $1,110
Cost of Implementation (Per Cluster Estimate) Project management: $2,080 Training and CME: Trainers: $ 450 Trainees: $15,120 Practice facilitation: $6,750 Quality circles: $ 900 PI visits: $2,700 Travel and food: $8,000 TOTAL: $36,000
Challenges and Caveats • Alcohol screening • How to comfortably and effectively ask • Who should do it • How often (every encounter?) • Alcohol treatment resources • Availability • Issues of confidentiality in small towns • Overweight and obesity • Lack of effective approaches • Insurance coverage of surgery • EHR limitations
Challenges and Caveats • Inadequate instruction and monitoring of exercise screening and interventions • Documentation issues in the practices