Download
1 / 1
10 likes | 269 Vues
Incidence and management of Shoulder Dystocia – a DGH perspective B. Alhindawi , Y. Abdallah , M. Elsayed Foda , A. Kothari. Obstetrics and Gynaecology Department. Hillingdon Hospital, London, United Kingdom. Objectives. Pre-partum risk factors.

E N D
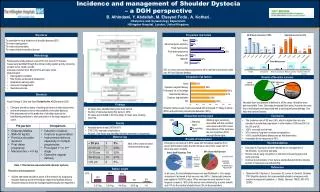
Incidence and management of Shoulder Dystocia – a DGH perspective B. Alhindawi, Y. Abdallah, M. ElsayedFoda , A. Kothari. Obstetrics and Gynaecology Department. Hillingdon Hospital, London, United Kingdom. Objectives Pre-partum risk factors To ascertain the local incidence of shoulder dystocia (SD) To review management To review documentation To review clinical neonatal outcomes. Methodology • Retrospective study between June 2010 and June 2011 inclusive. • Cases were identified through the clinical coding system and by reviewing incident forms, health records. • Data was collected from SD proforma and case notes. • Data included: • Demographic variables • Risk factors (antenatal & intrapartum) • Intrapartum warning signs. • Intra-event management. • Neonatal outcome. 50% of cases were post date pregnancies, 44% had fetal macrosomia, while only 9% had Diabetes Mellitus. Intrapartum risk factors Results of Neonatal outcome Standards • Royal College of Obst and GynaGuideline No. 42 December 2005. • Clinicians should be aware of existing risk factors in labouring women and must always be alert to the possibility of shoulder dystocia. • Risk assessments for the prediction of shoulder dystocia are insufficiently predictive to allow prevention of the large majority of cases. Neonatal team was present at delivery in all the cases. All babies were delivered within 7 min. One baby developed Erb’s palsy. However this case was a mild degree and responded well to subsequent physiotherapy. One baby had clavicle fracture. Findings Shoulder dystocia was mostly associated with prolonged 2nd stage of labour (56%) and performing instrumental deliveries (53%). • 40 cases were identified during the study period. • Number of deliveries during this period = 4472. • 34 cases are included in the final study. (6 notes were missing) • IUD 1/34. Intrapartum warning signs Conclusion Warning signs commonly associated with this condition were observed in 82% cases. Slow delivery of the head was the most common (35%) amongst these signs. • The incidence rate of SD was 0.9%, which is higher than the rate reported in unselected populations in older studies (1998 and 2001) in the US and UK. • 100% neonatal survival rate. • 97% cases no long-term neonatal complications. • 100% cases McRobertsManoeuvre as first intervention. • Immediate Senior response in 89%. Results • Neonatal survival rate (33/33)100 %. • 7/33 (21%) neonatal complications. • At least 1 risk factor was identified whether antenatal or intrapartum. Maternal age Results of management Recommendations Emergency call was put in 86% cases with immediate response from senior staff member within the first minute in about 90% cases half of them was senior midwife. Most of the cases revealed increased maternal age • Education & Training for all birth attendants for management of SD.(RCOG). by monthly skill drills. • Reduce risk by early recognition of risk factors & warning signs and early response. • Improve documentation of risk factors, standardized proforma, timeline & order of manoeuvres and debriefing. Table 1: Risk factors associated with shoulder dystocia. References Babies’ weight • Prevention and management: • All birth attendants should be aware of the methods for diagnosing shoulder dystocia and the techniques required to facilitate delivery. • Shoulder dystocia should be managed systematically(see Algorithm). • GhermanRB, Chauhan S, Ouzounian JG, Lerner H, Gonik B, Goodwin TM: Shoulder dystocia: the unpreventable obstetric emergency with empiric management guideline. J. Obstet. Gynecol. 195(3), 657–672 (2006). In all cases, the first attempted manoeuvre was McRobert’s . As a single manoeuvre it achieved a high success rate (48%). Supra-pubic pressure was applied in 18(53%) cases. Other manoeuvres were reported in less frequent occasions . 56% of the women were delivered by a senior midwife and 41% by the medical obstetric team (3% no documentation).