Geperforeerde Diverticulitis
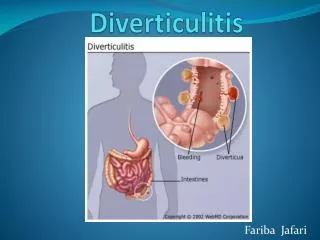
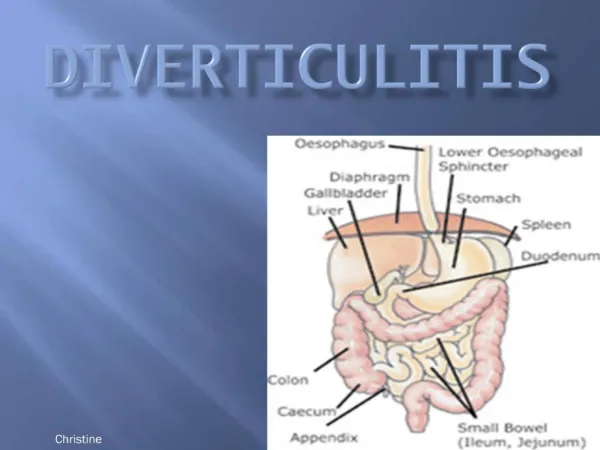
Geperforeerde Diverticulitis. Laparoscopische Lavage versus Sigmoidresectie. Diverticulitis. Divertikel: herniatie van mucosa, submucosa en serosa Diverticulosis coli: divertikels zonder symptomatologie Diverticulitis coli: ontsteking van divertikels (10-25%)


Geperforeerde Diverticulitis
E N D
Presentation Transcript
Geperforeerde Diverticulitis Laparoscopische Lavage versus Sigmoidresectie
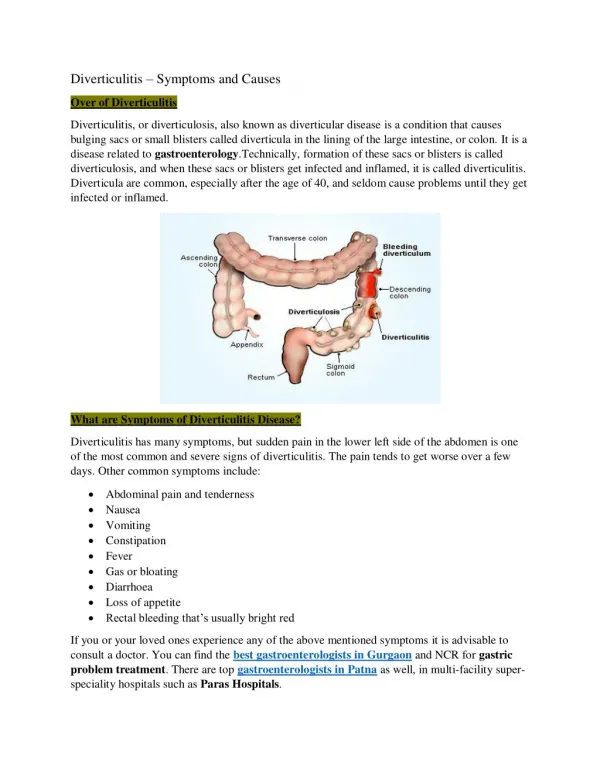
Diverticulitis • Divertikel: herniatie van mucosa, submucosa en serosa • Diverticulosis coli: divertikels zonder symptomatologie • Diverticulitis coli: ontsteking van divertikels (10-25%) • Gecompliceerde -itis (abces/fistelvorming/perforatie)
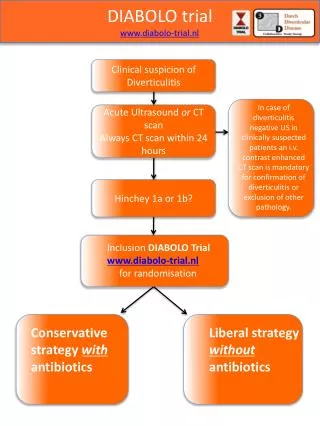
Diverticulitis • Hinchey classificatie • 0: klinisch milde diverticulitis • Ia: beperkte pericolische inflammatie • Ib: abces peri/mesocolisch <5cm nabij diverticulitis • II: abces retroperitoneaal of in kleine bekken • III: gegeneraliseerde purulente peritonitis (vrij lucht) • IV: faecale peritonitis
I Pericolic phlegmonwith small associatedabscess. II Large intra-abdominalabscess Hinchey classification of diverticulitis: Stage I: perforated diverticulitis with a confined paracolic abscess. Stage II: perforated diverticulitis with distant abscess formation. Stage III: noncommunicating perforated diverticulitis with fecal peritonitis Stage IV: perforation and free communication with the peritoneum, resulting in fecal peritonitis. III Small amounts of free air andfluid IV Massive pneumoperitoneum and free fluid Radiologische classificaties: CT-bevindingen gecorreleerd aan Hinchey scores
Behandeling Niveau 4 • Hinchey III/ IV • Algemeen: indicatie tot chirurgisch ingrijpen, afhankelijk van leeftijd, conditie en comorbiditeit • Standaard behandeling: Resectie Methods of surgical management of complicated diverticular disease. (1) Drainage, omental pedicle graft, and proximal diversion. (2) Hartman's procedure. (3) Sigmoid resection with coloproctostomy. (4) Sigmoid resection with coloproctostomy and proximal diversion.
Operatieve Therapie Niveau 2 • PRA vergelijkbare resultaten als HP(mits HD stabiele pt!) • Anastomose altijd combineren met lavagecolon en/of ontlastend stoma (mits ontledigdcolon) • morbiditeit (20-40%), mortaliteit (10-20%) • Laparoscopischeperitonealelavage & AB mogelijk lagere mortaliteit en morbiditeit
PICO • P: Patiënten met acute gecompliceerde diverticulitis (Gr. III/IV) • I: Laparoscopische Peritoneale Lavage • C: Resectie met primaire anastomose met/zonder deviërend stoma (RPA+/- DS) of Hartmann procedure (HP) • O: Effectiviteit, Morbiditeit & Mortaliteit
Zoek strategie • Pubmed, Cochrane Library, EMBASE, MEDLINE • Zonder taal restrictie • Restrictie: Humans, clinical trial, MA, RCT, clinicalstudy • Keywords: (’’Diverticulitis’’ [Mesh] OR ’’diverticulitis’’ [ Allfields]) AND (’’Laparoscopy’’ [AllFields] OR ’’peritonitis’’ [AllFields]) AND (’’Lavage’’ [AllFields] OR ’’laparoscopy’’ [AllFields])
Richtlijn 2012 Diagnostiek en behandeling acute diverticulitis van het colon • Level of Evidence: • Niveau 1: 2 onafhankelijke SR’s of meta-analyses • Niveau 2: RCT of 2 case-control studies • Niveau 3: 1 case-control of niet vergelijkend onderzoek • Niveau 4: mening van deskundige…..
Resultaten lavage • rerec
Conclusie • Laparoscopischeperitonealelavage & AB effectieve en veilige behandeling bij Hinchey III • Minimaal invasief, Morbiditeit 10,4%, Mortaliteit 1,7% • Onvoldoende bewijs bij Hinchey IV (niveau 4)
Discussie • Retrospectieve studies mogelijk lage methodologische kwaliteit • Ontbreken RCT’s • Selectiebias & publicatiebias • Ernst klinisch beeld • Gespecialiseerde centra • Leeftijd relatief laag • Heterogeniteit studies • Strategieën m.b.t. secundaire resectie (37,7%) verschilden per studie • Geen info over follow-up duur van alle studies (gem 38mnd)
Aanbevelingen • RCT waarin beide operatiestrategieën worden vergeleken: • April 2010 LADIES-TRIAL
Bronnen • RICHTLIJN DIAGNOSTIEK EN BEHANDELING ACUTE DIVERTICULITIS VAN HET COLON, 2012 • Alamili, M., Gogenur, I., Rosenberg, J. (2009). Acute complicated diverticulitis managed by laparoscopic lavage. Dis Colon Rectum.Jul;52(7), 1345-9. • Toorenvliet, B.R., Swank, H., Schoones, J.W., Hamming, J.F., Bemelman, W.A. (2010). Laparoscopic peritoneal lavage for perforated colonic diverticulitis: a systematic review. Colorectal Dis.Sep;12(9), 862-7 . • Abbas, S. (2007). Resection and primary anastomosis in acute complicated diverticulitis, a systematic review of the literature. Int J Colorectal Dis;22, 351-7 • Constantinides, V.A., Tekkis, P.P., Athanasiou, T., Aziz, O., Purkayastha, S., Remzi, F.H., Fazio, V.W. • (2006). Primary resection with anastomosis vs. Hartmann's procedure in nonelective surgery for • acute colonic diverticulitis: a systematic review. Dis Colon Rectum;49, 966-81. • Salem, L. & Flum, D.R. (2004). Primary anastomosis or Hartmann's procedure for patients with • diverticular peritonitis? A systematic review. Dis Colon Rectum;47, 1953-64. • Vermeulen, J., Akkersdijk, G.P., Gosselink, M.P., Hop, W.C., Mannaerts, G.H., van der Harst, E., Coene, • Zingg, U., Pasternak, I., Dietrich, M. Seifert, B., Oertli., D., Metzger, U. (2010). Primary anastomosis vs • Hartmann’s procedure in patients undergoing emergency left colectomy for perforated diverticulitis. Colorectal Disease, 12, 54–60.