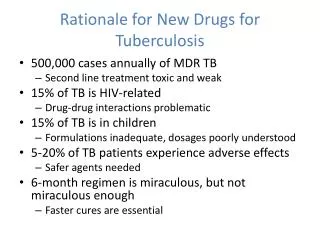
Rationale for Developing New Drugs
Nearly 25% of children diagnosed with cancer will not survive beyond five years, highlighting an urgent need for new therapeutic options. The acute toxicity of high-dose chemotherapy can be life-threatening, leading to long-term adverse effects such as growth delays, cognitive impairments, hormonal issues, and even secondary cancers. Pediatric clinical trials must recognize that children's cancer biology diverges significantly from adults, influencing drug disposition and sensitivity. This necessitates dedicated development and testing of molecularly-targeted drugs tailored to children's unique needs.

Rationale for Developing New Drugs
E N D
Presentation Transcript
Rationale for Developing New Drugs • 25% of children with cancer will not survive 5 years • The acute toxicity of dose-intensive chemotherapy is life-threatening • The long-term effects of cancer therapy can be debilitating or life-threatening • Growth delay • Cognitive effects • Hormonal/reproductive problems • Permanent tissue/organ damage • Second cancers
Toxicity in IRS-III Worst Degree of Any Toxicity (n=1062) No. of Patients Severity of Toxicity
Separate Pediatric Clinical Trials • Developmental changes affect: • Drug disposition (pharmacokinetics) • Tissue/organ sensitivity (pharmacodynamics) • Childhood cancers differ from adult cancers • Tissue of origin • Pathogenesis (genetic alterations) • Disease manifestations • Drug sensitivity
Pediatric vs. Adult MTD (1970s) MTDs in mg/m2 % Difference between Pediatric and Adult MTD
Pediatric vs. Adult MTD (1990s) % Difference between Pediatric and Adult MTD
New Agent Phase I Too Toxic Relapsed Phase II Inactive Relapsed Phase III Cured Not Efficacious Newly Diagnosed Approved Drug Clinical Anticancer Drug Development DRUGS PATIENTS
Docetaxel Phase I Trials * <500/µL for >7 days was considered dose-limiting
Determinants of Chemotherapy • Selection of front line treatment regimen • Tumor histology • Stage of cancer • Prognostic characteristics • Studying activity of new agents • Stratified by tumor histology
Molecularly-Targeted Drugs • Specific for molecular target (e.g., mutant ras) rather than histology • Patient treated based on presence of molecular lesion rather than tumor histology • Phase II trials not stratified by histology • Molecular pathogenesis of adult and childhood cancers different • Endpoint of dose finding (phase I) trials may be blocking target rather than toxicity • Toxicity profile and dose-limiting toxicity may be different than for cytotoxic agents