Download
1 / 1
10 likes | 91 Vues
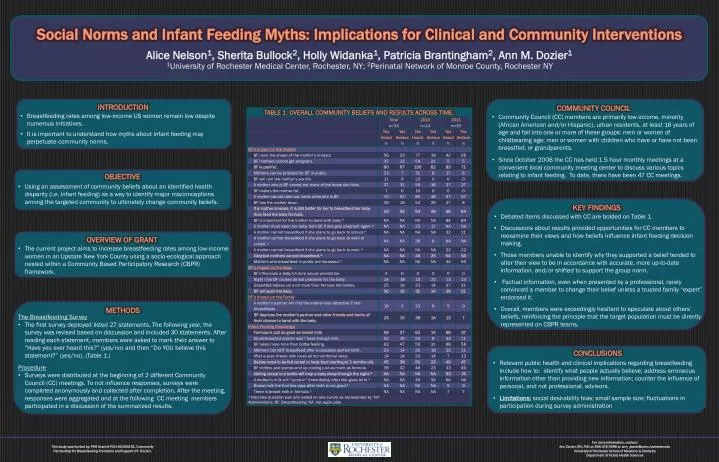
Social Norms and Infant Feeding Myths: Implications for Clinical and Community Interventions. Alice Nelson 1 , Sherita Bullock 2 , Holly Widanka 1 , Patricia Brantingham 2 , Ann M. Dozier 1.

E N D
Social Norms and Infant Feeding Myths: Implications for Clinical and Community Interventions Alice Nelson1, Sherita Bullock2, Holly Widanka1, Patricia Brantingham2, Ann M. Dozier1 1University of Rochester Medical Center, Rochester, NY; 2Perinatal Network of Monroe County, Rochester NY INTRODUCTION COMMUNITY COUNCIL • Breastfeeding rates among low-income US women remain low despite numerous initiatives. • It is important to understand how myths about infant feeding may perpetuate community norms. • Community Council (CC) members are primarily low-income, minority (African American and/or Hispanic), urban residents, at least 16 years of age and fall into one or more of these groups: men or women of childbearing age; men or women with children who have or have not been breastfed; or grandparents. • Since October 2008 the CC has held 1.5 hour monthly meetings at a convenient local community meeting center to discuss various topics relating to infant feeding. To date, there have been 47 CC meetings. OBJECTIVE • Using an assessment of community beliefs about an identified health disparity (i.e. infant feeding) as a way to identify major misconceptions among the targeted community to ultimately change community beliefs. KEY FINDINGS • Debated items discussed with CC are bolded on Table 1. • Discussions about results provided opportunities for CC members to reexamine their views and how beliefs influence infant feeding decision making. • Those members unable to identify why they supported a belief tended to alter their view to be in accordance with accurate, more up-to-date information, and/or shifted to support the group norm. • Factual information, even when presented by a professional, rarely convinced a member to change their belief unless a trusted family “expert” endorsed it. • Overall, members were exceedingly hesitant to speculate about others’ beliefs, reinforcing the principle that the target population must be directly represented on CBPR teams. OVERVIEW OF GRANT • The current project aims to increase breastfeeding rates among low-income women in an Upstate New York County using a socio-ecological approach nested within a Community Based Participatory Research (CBPR) framework. METHODS • The Breastfeeding Survey • The first survey deployed listed 27 statements. The following year, the survey was revised based on discussion and included 30 statements. After reading each statement, members were asked to mark their answer to “Have you ever heard this?” (yes/no) and then “Do YOU believe this statement?” (yes/no). (Table 1.) • Procedure • Surveys were distributed at the beginning of 2 different Community Council (CC) meetings. To not influence responses, surveys were completed anonymously and collected after completion. After the meeting, responses were aggregated and at the following CC meeting members participated in a discussion of the summarized results. CONCLUSIONS • Relevant public health and clinical implications regarding breastfeeding include how to: identify what people actually believe; address erroneous information other than providing new information; counter the influence of personal, and not professional, advisors. • Limitations:social desirability bias; small sample size; fluctuations in participation during survey administration For more information, contact:Ann Dozier, RN, PhD at 585-276-3998 or ann_dozier@urmc.rochester.edu University of Rochester School of Medicine & DentistryDepartment of Public Health Sciences This study was funded by: PHS Grant # RO1-HD055191, Community Partnership for Breastfeeding Promotion and Support (PI: Dozier).