ARTHROPODA Class ARACHNIDA
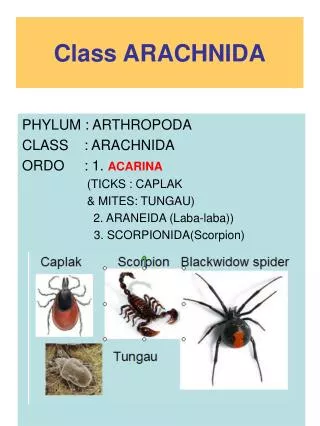
ARTHROPODA Class ARACHNIDA. Doç.Dr.Hrisi BAHAR. Phylum Arthropoda. Subphylum CRUSTACEAE ● Class Arachnida ● Class Insecta. Class Aracnida. ----------------------------------------------------------. Prostigmata. Mesostigmata. Mites Cheyletiella, Neotrombicula. Metastigmata. Mites

ARTHROPODA Class ARACHNIDA
E N D
Presentation Transcript
ARTHROPODA Class ARACHNIDA Doç.Dr.Hrisi BAHAR
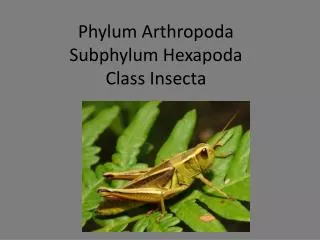
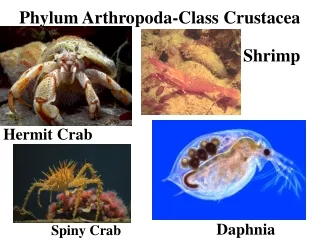
Phylum Arthropoda • Subphylum CRUSTACEAE ●Class Arachnida ●Class Insecta
Class Aracnida ---------------------------------------------------------- Prostigmata Mesostigmata Mites Cheyletiella, Neotrombicula Metastigmata Mites Dermanyssus Rnithonyssus Ticks Family Ixodidae Ixodes Dermacentor Rhipicephalus, Haemaphysalis Family Argasidae Argas, Ornithodoros Astigmata Mites Sarcoptes, Notoedres, Psoroptes,Tyrophagus, Tyroglyphus, Glyciphagus, Dermatophagoides
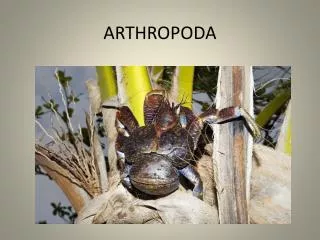
ArachnidaTicks (Ixodida) ●They are blood-sucking, opportunistic parasites that can attach to the skin of a variety of vertebrate hosts. ● They have no segmentation and are dorso-ventrally flat with four pairs of legs
●All stages of the tick life cycle can suck blood, it is normally the adult tick that poses a problem for humans. • The order metastigmata includes two important families, • Argasidae (soft ticks) • Ixodidae (hard ticks) • The latter is the most significant group worldwide
●Approximately 20 hard tick species are indigenous to western and central Europe, belonging to the genera Ixodes, Rhipicephalus, Dermacentor, andHaemaphysalis. ●The most important species is Ixodes ricinus that accounts for about 90% of the tick fauna in this region.
Ixodes ricinus • ●Vector of the causative agents of Lyme borreliosis and Tickborne encephalitis • ● Human tick bites in central Europe are in most cases caused by I. ricinus and only occasionally by other tick species.
Morphology. • Male: About 2–3mm long with a highly chitinized scutum covering the entire dorsal surface. Female: 3–4mm, up to 12mm when fully engorged after a blood meal; the scutum covers only the anterior portion of the body. • .
female male
●Adults and nymphs have four pairs of legs, the smaller larvae (about 0.5mm long)has only three pairs of legs ●Ticks possess characteristic piercing mouthparts.
Life cycle Eggs Larva Nymph Male Female Life cycle
● The various stages of I. ricinus are dependent on blood meals from vertebrates throughout their developmental cycle. Having selected a suitable location on a host, a female tick inserts her piercing mouthparts into the skin within about 10 minutes. • ● Using clawlike organs at the tip of stylettelike • mouthparts, the chelicerae, the tick cuts a wound into which the unpaired,barbed, pinecone-shaped hypostome is then inserted to anchor the parasite in the skin.
●While sucking blood, ticks secrete large amounts of saliva,containing cytolytic, anticoagulative, and other types of substances. They ingest blood, tissue fluid and digested tissue components. ● The weight of the female increases considerably during a blood meal. When completely engorged the tick resembles a ricinus seed. Ixodes ricinus female engorged with blood
Epidemiology The epidemiologically important factor is the possible ingestion of pathogens with the blood meal, which can, at a following blood meal in the tick’s next developmental stage, be inoculated into another vertebrate host (horizontal transmission). Female ticks even transmit certain pathogens by the transovarial route to the next generation of ticks (vertical transmission).
Developmental stageHost groups commonly used for blood feeding Egg -- Larva Rodents,birds,humans Nymph Birds,mamals,human Imago(Adult) Domestic and wild ruminants,dogs, cats,horses, and other animal species,humans
The great epidemiological significance of I.ricinus in central Europe is predominantly due to its function as vector of the causative agents of Lyme borreliosis(Borrelia burgdorferi ) and the European tickborne encephalitis (TBE) In northern and eastern Europe the TBE virus is transmitted by Ixodes persulcatus.
DISEASES FOR WHICH HARD TICKS ARE CARRIERS BACTERIAL DISEASES Rocky Mountain Spotted Fever The causative agent,Ricketsia rickettsii, is carried by the Brown Dog tick and the Rocky Mountain Wood Tick (the two Dermacentor species )
DISEASES FOR WHICH HARD TICKS ARE CARRIERS BACTERIAL DISEASES Tularemia One of the several ways that humans can be infected is by being bitten by a tick that has acquired the bacterium after biting one of a rodent carryıng Francisella tularensis
DISEASES FOR WHICH HARD TICKS ARE CARRIERS BACTERIAL DISEASES Q Fever Various farm animals (cattle sheep goats etc) are the primary carriers of the bacterium Coxiella burnetii which causes Q fever. Spread to humans is usually via inhalation of dust containing dried urine, feces etc of infected animals. However, less commonly, the bacterium can be transmitted via the bite of Dermacentor ticks .
Q Fever Clinical manifestation Acute Q fever Many patients, about half, show no signs of infection but in others after an incubation period of 1 - 2 weeks, there is a sudden onset of fever, headache, general malaise, myalgia, sore throat, chills, sweats, non-productive cough, nausea, vomiting, diarrhea, abdominal pain, and chest pain. The patient may also appear confused. Many patients go on to the symptoms of pneumonia and hepatitis but most recover in a month or two without treatment although acute Q fever has a mortality rate of 1-2%.
Q Fever Chronic Q fever If the patient fails to resolve the infection, chronic Q fever results. This can occur a few months after primary infection but can also occur many years later. Endocarditis of the aortic heart valves is the major problem that arises. This usually occurs in people with heart valve disease but also at risk are transplant, cancer and kidney disease patients. The chronic form of Q fever has a fatality rate of about 60 - 70%.
Q Fever Diagnosis Serology to determine the presence of antibodies against Coxiella burnetii is used. Treatment Antibiotics such as doxycyline are used to treat acute Q fever. For chronic Q fever, two protocols have been İnvestigated doxycycline along with quinolones for at least 4 years and doxycycline with hydroxychloroquine for 1.5 to 3 years. There is a vaccine used in Australia for persons who may come in contact with C. burnettii but it is not commercially available in the United States.
DISEASES FOR WHICH HARD TICKS ARE CARRIERS BACTERIAL DISEASES Human erlichiosis is carried by Dermacentor variabilis and by Amblyomma americanum and is caused by a number of bacteria of the Ehrlichia family . As with many tick-borne diseases, incidence follows vector distribution with higher incidence during the summer months when tick populations and contact with them are higher .
DISEASES FOR WHICH HARD TICKS ARE CARRIERS BACTERIAL DISEASES Lyme Dısease Lyme disease is caused by the spirochete bacterium, Borrelia burgdorferi which typically infects small mammals in the northeast and north central United States. It is transmitted to humans by Ixodid black legged ticks . There are over 20,000 cases per year in the United States making it the most common tick-borne disease in North America. In Europe, a similar disease is caused by Borrelia garinii or Borrelia afzelii.
Lyme Disease Clinical manifestation Fever, headache and malaise and characteristic rash named erythemia migrans which can occur in a few days but sometimes only after a few weeks, are typical of Lyme Disease. The rash often has a bull’s eye appearance since as it grows ,the central region clears. If left untreated, the infection spreads and can result in Bell’s Palsy(partial paralysis of muscles in one or both sides of the face), meningitis, heart palpitations and severe joint pain.
Lyme Disease These symptoms usually resolve in a few weeks but after several months about 60% of patients will get severe joint swelling and arthritis. A small minority may also get neurologic symptoms. Diagnosis Various laboratory tests include Elisa, Western blot
Lyme Disease Treatment Early administration with antibiotics (doxycycline, amoxicillin, or cefuroxime axetil) is recommended. Some patients continue with neurological and muscle pain problems even after antibiotic treatment. It is not known what causes these but they may be autoimmune in nature.
DISEASES FOR WHICH HARD TICKS ARE CARRIERS VIRAL DISEASES Crimean-Congo Hemorrhagic Fever Caused by a Nairovirus, a member of the Bunyaviridae. It is found in Eastern Europe and throughout the Mediterranean areas of southern Europe, the Middle East, Africa,China central and south Asia..
Crimean-Congo Hemorrhagic Fever Ixorid ticks (genus Hyalomma) spread the virus, which is also carried by numerous species of domestic and wild animals.Person to person transmission Through infected blood and other body fluids hasbeen documented.
Crimean-Congo Hemorrhagic Fever Clinical manifestation Initially, the patient presents with headache, high fever, back pain, joint pain, stomach pain, and vomiting. There may be flushing, red eyes and throat and small red spots called petechiae on the palate. Hemorrhage ensues after a few days and lasts for a few weeks . This is indicated by severe bruising, nosebleeds, and failure to stop bleedings after a cut or injection. Slow recovery often ensues but mortality can be as high as 50%.
Crimean-Congo Hemorrhagic Fever Treatment Since this is a viral disease, Treatment is largely supportive with particular attention to electrolyte balance. Ribavirin has been used. An inactivated vaccine has been used in Eastern Europe.
Crimean-Congo Hemorrhagic Fever Virus in High-Risk Population, Turkey • In the Tokat and Sivas provinces of Turkey, the overall Crimean-Congo hemorrhagic fever virus (CCHFV) seroprevalence was 12.8% among 782 members of a high-risk population. CCHFV seroprevalence was associated with history of tick bite or tick removal from animals, employment in animal husbandry or farming, and being >40 years of age. Turabi Gunes, Aynur Engin, Omer Poyraz, Nazif Elaldi, Safak Kaya, Ilyas Dokmetas, Mehmet Bakir, and Ziynet CinarCumhuriyet University, Sivas, Turkey • CDC March 2009
DISEASES FOR WHICH HARD TICKS ARE CARRIERS VIRAL DISEASES Tıck -Born Encephalitis This disease results from infection by tick-borne encephalitis virus, which is a member of the Flaviviridae. Clinical manifestation Tick-borne encephalitis starts as mild influenza-like symptoms with fever accompanied by leuko and trombocytopenia. This resolves within a few days. However, about one third of patients develop meningitis and meningoencephalitis. This can, in a few cases, be followed by paralysis.
Tıck -Born Encephalitis The European form of the disease has a mortality rate of under 5%. Most patients recover but about a third may have long lasting Neurological problems. Treatment Supportive is indicated. There is an experimental killed vaccine in Europe. In Sweden TBE vaccination is recommended for residents of and regular visitors to TBE endemic areas.
Tick bite prevention • Tick habitats with dense undergrowth, ferns, and high grasses should be avoided as far as possible. If this is unavoidable, proper clothing must be worn: shoes, long socks, long trousers (tuck legs of trousers into socks), long sleeves that fit closely around the wrists. • Additional protection is provided by spraying the clotheswith acaricides, especially pyrethroids,which havea certain repellent effect (e.g., flumethrin). The effect of repellents applied to the skin (for malaria) is in most cases insufficient to protect against ticks.
Tick bite prevention • After staying in a tick habitat persons should search their entire body for ticks and remove any found attached to the skin as quickly as possible by mechanical means (do not apply oil or other substances to attached ticks
Tick bite prevention • Any bites should be watched during the following four weeks for signs of reddening (erythema), swelling, and inflammation. • A “migrating,” spreading rash (erythema migrans) is indicative for a Borrelia infection. • On the other hand, this sign is not observed in all infected persons.
Mites Sarcoptes scabieiCausative agent of scabies Scabies mite (Sarcoptes scabei) is the cause of scabies and is distributed worldwide. Epidemics of the disease may occur for long periods but mites may be common at all times in very poor communities with inadequate washing facilities.
Life cycle Egg Larva Nymph Adult Life cycle of the Scabies mite (Sarcoptes scabei)
Sarcoptes scabei 1-Females deposit eggs at 2 to 3 day intervals as they burrow through the skin . Eggs are oval and 0.1 to 0.15 mm in length and incubation time is 3 to 8 days. 2-After the eggs hatch, the larvae migrate to the skin surface and burrow into the intact stratum corneum to construct almost invisible, short burrows called molting pouches.
Sarcoptes scabei 3-The larval stage, which emerges from the eggs, has only 3 pairs of legs , and this form lasts 2 to 3 days. After larvae molt, the resulting nymphs have 4 pairs of legs . This form molts into slightly larger nymphs before molting into adults. 4-Larvae and nymphs may often be found in molting pouches or in hair follicles and look similar to adults, only smaller.
Sarcoptes scabei Adults are round, sac-like eyeless mites. Females are 0.3 to 0.4 mm long and 0.25to 0.35 mm wide, and males are slightly more than half that size. Mating occurs after the male penetrates the molting pouch of the adult female
Sarcoptes scabei • Impregnated females extend their molting pouches into the characteristic serpentine burrows, laying eggs in the process. The impregnated females burrow into the skin and spend the remaining 2 months of their lives in tunnels under the surface of the skin. Males are rarely seen. They make a temporary gallery in the skin.
Sarcoptes scabei • Epidemiology. • Transmission is by close contact (sexual partners, family,members, school children, healthcare staff) from person to person, • Indirect transmission on clothes (underclothes), bed linens is not a primary route, but should be considered as a factor in control measures. • Without a host, mites usually die off within a few days. Mite infections can also be acquired from animals to which humans have close skin contact.
Sarcoptes scabei Clinical manifestations. An early sign of an initial infestation with Sarcoptes mites is the primary efflorescence with mite tunnels up to 2–4mm and sometimes 10 mm long threadlike, irregularly . The female mite is found at the end of the burrow in a small swelling. Following an inapparent period of about four to five weeks, during whith time a hypersensitivity response to mite antigens develops
Sarcoptes scabei • The scabies exanthema manifests in the form of local or generalized pruritus, which is particularly bothersome in the evening when body heat is retained under the bedcovers. • The evolving skin lesions are papulous or • apulovesicular exanthema and reactions due to scratching. • In adults, these lesions are seen mainly in the interdigital spaces and on the sides of the fingers, on the wrists and ankles and in the genital region. Children also occasionally show facial lesions.