Tobacco Cessation During Pregnancy: Prevalence and Interventions Van Tong, MPH Epidemiologist, CDC Division of Reprodu
U.S. Department of Health and Human Services Centers for Disease Control and Prevention Tobacco Cessation During Pregnancy: Prevalence and Interventions Van Tong, MPH Epidemiologist, CDC Division of Reproductive Health October 21, 2009 CDC Division of Reproductive Health (DRH)

Tobacco Cessation During Pregnancy: Prevalence and Interventions Van Tong, MPH Epidemiologist, CDC Division of Reprodu
E N D
Presentation Transcript
U.S. Department of Health and Human Services Centers for Disease Control and Prevention Tobacco Cessation During Pregnancy: Prevalence and Interventions Van Tong, MPHEpidemiologist, CDC Division of Reproductive HealthOctober 21, 2009
CDC Division of Reproductive Health (DRH) Our mission is to promote optimal reproductive and infant health and quality of life by influencing public policy, health care practice, community practices, and individual behaviors through scientific and programmatic expertise, leadership, and support. http://www.cdc.gov/reproductivehealth/
DRH work in tobacco use & pregnancy • Monitor trends of tobacco use before, during and after pregnancy • Conduct research on health outcomes & economic costs • Evaluate interventions and promote effective interventions and policies • Provide technical assistance to organizations http://www.cdc.gov/reproductivehealth/TobaccoUsePregnancy/
Presentation outline • Prevalence and trend of prenatal tobacco use • Overall • Among pregnant teens • Review recommendations for screening and treatment for tobacco cessation among pregnant women • Provide cessation resources
Health effects (1) Prenatal smoking is one of the most common preventable causes of poor birth outcomes Smoking among women causes • Reduced fertility • Preterm delivery • Restricted fetal growth • Preterm-related deaths and SIDS Second hand smoke (SHS) exposure • Respiratory tract infections and SIDS Source: Surgeon General’s Report: The Health Consequences of Smoking, 2004
Risks of maternal smokeless tobacco use less studied However, data suggest an increased risk of Stillbirth Low birth weight Prematurity Preeclampsia Infant death Health effects (2)
Percent of mothers who smoked during pregnancy in US, birth certificates 1990 – 2005* 2003 revised birth certificate implemented Percent * Source: Birth certificates, National Center for Health Statistics; excludes California. Not all states had data for the entire observation period
Percent of mothers who smoked during pregnancy in US, birth certificates 1990 – 2003* Percent * Source: Birth certificates, National Center for Health Statistics; excludes California.
Prenatal smoking reported on 2003 US birth certificates by state > 16% 12-16% 8-11% <8% State-specific range was 3.5% (DC) to 26.1% (WV). Source: CDC SAMMEC: http://apps.nccd.cdc.gov/sammec/
Smoking 3 months before pregnancy among live births in 25 PRAMS states* by maternal race/ethnicity and age, 2005 * AK, AR, CO, FL, GA, HI, IL, ME, MD, MI, MN, NE, NJ, NM, NY (includes NYC), NC, OH, OK. OR, RI, SC, UT, VT, WA, WV
Smoking during pregnancy among live births in 25 PRAMS states* by maternal race/ethnicity and age, 2005 * Smoking ascertained from PRAMS and linked birth certificate. AK, AR, CO, FL, GA, HI, IL, ME, MD, MI, MN, NE, NJ, NM, NY (includes NYC), NC, OH, OK. OR, RI, SC, UT, VT, WA, WV
Smoking after delivery among live births in 25 PRAMS states* by maternal race/ethnicity and age, 2005 * On average 4 months after delivery. AK, AR, CO, FL, GA, HI, IL, ME, MD, MI, MN, NE, NJ, NM, NY (includes NYC), NC, OH, OK. OR, RI, SC, UT, VT, WA, WV
Trends in prenatal smoking among teens • Teens smoke more than any other age groups (1990-2002), but the rates may have fallen more in recent years1 • Decreased from 20.3% in 1990 to 17.1% in 2002. • 15 out of 45 states had significant increases in teen smoking during pregnancy from 1995-2002. • Tobacco use associated with other higher risk behaviors • Many young persons engage in sexual risk behavior and experience negative reproductive health outcomes2 1 CDC. Smoking during pregnancy--United States, 1990-2002. MMWR. 2004 Oct 8;53(39):911-5. 2 Gavin et al. Sexual and reproductive health of persons aged 10-24 years - United States, 2002-2007. MMWR Surveill Summ. 2009 Jul 17;58(6):1-58.
Tobacco use before, during, after pregnancy among Alaska Native and white women in Alaska, PRAMS 2000-2003 Source: Kim et al. Patterns of Cigarette and Smokeless Tobacco Use Before, During, and After Pregnancy Among Alaska Native and White Women in Alaska, 2000–2003. Matern Child Health J. 2009 Jan 13.
Natural history of smoking during pregnancy • 25%-50% spontaneously quit smoking after learning of pregnancy(Floyd et al., 1993; LeClere & Wilson, 1997; Severson et al., 1995; Tong, 2008) • Another 12% quit later on; however, the majority of pregnant smokers cut down, but do not quit (Fingerhut et al., 1991) • Of women who quit during pregnancy, about 70% relapse within 1 year following delivery (Fingerhut et al., 1991)
Benefits of cessation • Early cessation is best: • Women quit quit smoking by 16 weeks gestation have normal birth weight infants (MaCarther et al, 1988) • Women who quit smoking by 30-36 weeks have near normal birth weight infants (Ahlsten et al., 1993) • Women who quit smoking by 15 weeks, rates of spontaneous preterm birth and small for gestational age infants did not differ from those in non-smokers (McCowan 2009) • Compared with women who smoked throughout pregnancy, first-trimester quitters reduced their odds of delivering(Polakowski 2009): • preterm non-SGA newborn by 31% • term SGA newborn by 55% • preterm SGA newborn by 53%
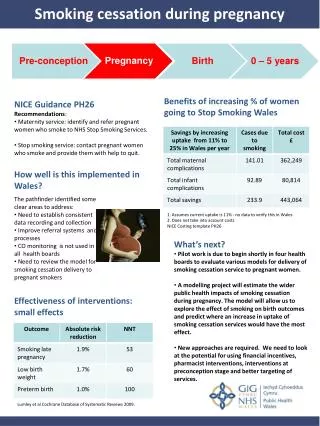
2008 USPHS recommendations for pregnant smokers • Because of the serious risks of smoking to the pregnant smoker and the fetus, whenever possible pregnant smokers should be offered person-to-person psychosocial interventions that exceed minimal advice to quit. (Strength of Evidence = A) • Although abstinence early in pregnancy will produce the greatest benefits to the fetus and expectant mother, quitting at any point in pregnancy can yield benefits. Therefore, clinicians should offer effective tobacco dependence interventions to pregnant smokers at the first prenatal visit as well as throughout the course of pregnancy. Fiore et al., http://www.ncbi.nlm.nih.gov/books/bv.fcgi?rid=hstat2.chapter.28163
Pharmacotherapy • Pregnancy quit rates rarely exceed 18% • Pharmacotherapies double quit rates in non-pregnant women • Not enough information on the efficacy and safety of pharmacotherapies during pregnancy, so unable to assess benefit/risk (Fiore 2008) • Psychosocial interventions should be first treatment option among pregnant smokers (Oncken, Nicotine Tob Res, 2009) • More research needed on pharmacotherapies for cessation and pregnancy
5A’s model for tobacco cessation Ask about tobacco use. Identify and document tobacco use status for every patient at every visit. Adviseto quit. In a clear, strong and personalized manner urge every tobacco user to quit. Quitting early in pregnancy provides the greatest benefit to the fetus Assess willingness to make a quit attempt. Is the tobacco user willing to make a quit attempt at this time? Assistin quit attempt. For the patient willing to make a quit attempt, offer medication and provide or refer for counseling or additional treatment to help the patient quit.For patients unwilling to quit at the time, provide interventions designed to increase future quit attempts. Arrangefollowup. For the patient willing to make a quit attempt, arrange for follow-up contacts, beginning within the first week after the quit date.For patients unwilling to make a quit attempt at the time, address tobacco dependence and willingness to quit at next clinic visit.
Screening for Tobacco Use in Pregnant Women • Assess pregnant women’s smoking status using a multiple-choice question to improve disclosure (Fiore et al., Table 7.7, 2008) • I smoke regularly now; about the same as before finding out I was pregnant • I smoke regularly now; but I cut down after finding out I was pregnant • I smoke every once and awhile • I have quit smoking since finding out I was pregnant. • I wasn't smoking around the time I found out I was pregnant, and I don't currently smoke cigarettes.
Relapse prevention • Two meta-analyses of relapse prevention trials (both pre- and post-delivery) found no significant reduction in relapse. • Postpartum relapse may be decreased by continued emphasis on the relationship between maternal smoking and poor health outcomes in infants and children (e.g., SIDS, respiratory infections, asthma, and middle ear disease) Fiore et al, 2008
Clinical interventions part of comprehensive tobacco control • Clinic-based interventions have limited impact • Universal implementation would only reduce prevalence by 0.8% (16.7% to 15.9%) (Kim et al 2009) • Prenatal smokers harder to reach or treat • Young, less educated, uninsured • Heavier smokers • Comprehensive tobacco control programs and policies (taxes, smoke-free laws, etc…) • For example, cigarette taxes have an effect in reducing prenatal smoking rates (Ringel 2001, Colman 2003)
Telephone-based quitlines • Quitlines eliminate barriers of access for women • Free Services • No transportation required • Convenient and hours flexible • Trained Staff • Funded by CDC • Available in all US states and territories • National portal number (1-800-QUIT-NOW or 1-800-784-8669) • All state QL have specialized materials for pregnant women; some are implementing postpartum counseling sessions
What do we know about telephone counseling and pregnant smokers? Evidence suggests that telephone counseling is effective, especially for light smokers (<10 cig a day) and for women who have already attempted to quit (McBride et al study AJPH 1999; Rigotti et al study Obstet & Gyn 2006;CA evaluation of quitlines among pregnant smokers)
Medicaid coverage of tobacco treatments • Women enrolled in Medicaid have a smoking prevalence 3 times greater than prevalence among women who are privately insured (23.5% vs 7.9%) • 7 state Medicaid programs (CA, IN, MN, NY, OR, PA, WV) cover all tobacco medications and one form of counseling, and 39 programs covered at least one form of treatment* *CDC. State Medicaid coverage for tobacco-dependence treatments--United States, 2006. MMWR 2008 Feb 8;57(5):117-22. http://www.cdc.gov/mmwr/preview/mmwrhtml/mm5705a2.htm
Resources For consumers • Info on smoking and pregnancy: http://www.cdc.gov/Features/PregnantDontSmoke/ • Tips on quitting: http://women.smokefree.gov/ • Smoke free home pledge: http://www.epa.gov/smokefree/ • 1-800-QUIT-NOW: http://1800quitnow.cancer.gov/ For clinicians and public health practitioners • ACOG Clinician guide to helping pregnant women quit smoking: http://www.acog.org/departments/dept_web.cfm?recno=13 • National Partnership for Smoke-free Families, consumer and practitioner resources: http://smokefreefamilies.tobacco-cessation.org/ • Clean Air for Healthy Children: www.cleanairforhealthychildren.org
National Partnership for Smoke-free Families • Clinician and consumer materials • Native American Action Plan: tailor 5A’s for American Indian populations • Medicaid Toolkit: health and economic costs and benefits of coverage, state activities • Community and Worksite Toolkit: for employers • http://smokefreefamilies.tobacco-cessation.org/
http://www.cdc.gov/mmWR/PDF/ss/ss5804.pdfFree hard-copies available upon request
Summary • Prenatal smoking rates declining in US, but disparities continue to exist • Pregnant teens have high rates of smoking before, during, and after pregnancy • Brief counseling and pregnancy-specific materials are effective for prenatal smoking cessation • Coverage of cessation may be covered by Medicaid or can be accessed for free through state-based quitlines
Contact information Tobacco Use and Pregnancy Website: http://www.cdc.gov/reproductivehealth/TobaccoUsePregnancy/index.htm Van Tong Vtong@cdc.gov 770-488-6309