Download
1 / 51
530 likes | 743 Vues
The Evolutionary Biology of Human Fetal and Childhood Development (1) Brief review of relevant theory (2) Stages of fetal and childhood development (3) Maternal-offspring interactions at each stage

E N D
The Evolutionary Biology of Human Fetal and Childhood Development (1) Brief review of relevant theory (2) Stages of fetal and childhood development (3) Maternal-offspring interactions at each stage (4) Maternal-offspring conflicts, other evolutionary considerations such as ancestral-modern mismatches, and their potential effects on health
Evolutionary theory for maternal-offspring interactions Parties involved, (one INSIDE the other), and how they maximize their inclusive fitness Genes in mother - selected for effects that maximize inclusive fitness of the mother, via equal investment in offspring with same benefits and costs, & via more investment in ‘better’ offspring, less investment in ‘worse’ ones. Are tradeoffs between current and future offspring, and between offspring quantity and quality. Assume that specific alleles in mother cannot recognize copies of themselves in a given offspring (‘green-beard’ or ‘intergenerational epistasis’ effect) (2) Genes in fetus, child Non-imprinted genes - selected to take more from mother than she is selected to provide, up to the point that costs to sibs become too great
Evolutionary theory for maternal-offspring interactions Parties involved, and how they maximize their inclusive fitness (2) Genes in fetus, child Paternally-expressed imprinted genes - gene ‘knows’ it is paternally-inherited, has less chance of being in sibs, so exerts relatively more demands on mother compared to Maternally-expressed imprinted genes - gene ‘knows’ it is maternally-inherited, has equal chance of being in sibs, so exerts relatively less-selfish effects on mother This is intragenomic conflict within the fetus, child. How is it resolved, or not?! Historically, there has been selection for silencing by mother (in oogenesis) of genes that enhance offspring growth, and silencing by father (in spermatogenesis) of genes that reduce offspring growth -> this system evolved in concert with origin of placental mammals
Evolutionary theory tells us about conflicts, confluences of interest But to understand outcomes, we also need information on who is in control of what aspects of the interaction -tug of war, dynamic equilibrium -one side ‘wins’, resulting in disease in other -both sides can lose, resulting in disease, if mechanisms go awry -conflict costs
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Invasion of the placenta • Maternal-fetal food fights (a) Glucose concentration (b) Blood supply • Gestation length • Survival of the fattest and cutest • Sucking, crying, weaning, whining • Survival and increased reproduction of the slower-developing child
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Mother undergoes menstruation (shedding of uterine lining with visible loss of blood) every month by default. Such menstruation is very rare in mammals, found only in a few species with invasive placentation. There is a continuum between menstruation, early miscarriage, premature delivery, shedding of placenta at parturition ADAPTIVE SIGNIFICANCE OF MENSTRUATION? Menstruation may be a pre-emptive defense against excessive placental invasion, and/or an evolved mechanism for selective early embryo elimination (many other mammals just resorb unwanted embryos) Eliminate defective embryo (if extrinsic conditions are ok), or any embryo (if extrinsic conditions are poor)
Eliminate defective embryos (if extrinsic conditions are ok), or any embryos (if extrinsic conditions are poor) IMPLICATIONS FOR HUMAN FERTILITY & INFERTILITY?
Eliminate defective embryos (if extrinsic conditions are ok), or any embryos (if extrinsic conditions are poor) Early embryo loss is very very common in humans (>30% of conceptions are lost in first few weeks, 10-20% of remainder are lost in first few months; most miscarriages have chromosomal abnormalities) COSTS AND BENEFITS TO MATERNAL AND FETAL GENES, of embryo loss? Mother COST: one-month delay BENEFIT: avoid pregnancy in poor conditions, or raising low-fitness offspring -> selects for maternal screening of embryo quality/vigor (2) Fetus COST: death BENEFIT: if low-fitness enough, gain in inclusive fitness via effects on mother (adaptive suicide) -> selects for mechanisms that maintain the pregnancy Human chorionic gonadotropin (hCG) may have originatedto help maintain the pregnancy, when mother would otherwise abort it, may be maintained, with maternal response to the hormone, as signal of embryo quality
First invasion (start of pregnancy): implantation deep in uterine tissue Second invasion (near end of 1st trimester): formation of placenta itself
Stages of Maternal-Offspring interactions (2) Invasion of the placenta Conceptus free in lumen of uterus for about a week, implants, nourished without placenta for most of 1st trimester, then placenta develops from fetal extra embryonic tissue, in late first trimester MOTHER: spiral arteries develop, to supply placenta, fetus with blood; tough tough endometrial matrix develops, first around spiral arteries FETUS: placental tissue invades spiral arteries, remodels them into large-diameter, low-resistance vessels CONSEQUENCES: Fetus gains direct access to maternal arterial blood. Mother cannot reduce nutrient content of blood reaching placenta without reducing nutrient supply to her own tissues Volume of blood reaching placenta cannot be restricted by mother Placenta can release hormones and other substances directly into mother’s blood, and monitor the content of mother’s blood
(3) Maternal-fetal food fights: (a) Glucose concentration (b) Blood supply Maternal fasting blood sugar (‘set point’) is reduced, starting in early pregnancy. Later in pregnancy, maternal glucose and maternal insulin are higher after a meal than in non-pregnant state. Mother and fetus compete after each meal for share of glucose in blood. The longer it takes mother to reduce her blood sugar, the bigger the share for the fetus Human placental lactogen (hPL), released in very large quantities (perhaps via ‘arms race’ of signals & responses) by the placenta, acts on the mother’s prolactin receptors to increase maternal resistance to insulin. hPL causes blood sugar to remain higher after a meal hPL is not essential for a successful pregnancy. To counter the effects of hPL, mothers produce an increased amount of insulin. Gestational diabetes can result if mother cannot mount adequate response to fetal manipulation. Babies of mothers with gestational diabetes are big and fat.
Gestational diabetes: high blood glucose in pregnancy Affects about 10% of pregnancies Generally has few overt symptoms Caused by placental hormones Hallmark is increased insulin resistance: have plenty of insulin, but insulin receptor-based cell signaling pathways are not activated properly (5) Resolves once the baby is born (6) RISKS: (a) macrosomia (baby too big) and birth difficulties, metabolic imbalance in neonate (neonate keeps high insulin levels, develops low blood sugar), (c) increased risk of type 2 diabetes in mother and in child, in later life, and obesity in the child.
A placental lactogen gene is imprinted (and paternally-expressed) in mice
Placental lactogen (CSH) genes evolve under positive selection(have also duplicated often)
(3) Maternal-fetal food fights: (a) Glucose concentration (b) Blood supply As you recall: MOTHER: spiral arteries develop, to supply placenta, fetus with blood; tough tough endometrial matrix develops, first around spiral arteries FETUS: placental tissue invades spiral arteries, remodels them into large-diameter, low-resistance vessels Mother cannot restrict blood supply to placenta Can offspring increase it? Only way is to increase maternal blood pressure Conflict over blood supply should increase over course of gestation, since (1) nutrient requirements increase and (2) size of placenta (the source of fetal ‘power’) increases (1) Maternal blood pressure decreases in early to mid pregnancy (apparent maternal adaptation to reduce fetal share of blood) (2) Progressive rise in maternal blood pressure towards term -> may result in pre-eclampsia; Is it due to the fetus?
Pre-eclampsia: combination of pregnancy-induced hypertension and proteinuria (protein in urine due to lesions in kidney blood vessels) End of continuum of blood pressure, many different causes, no cure aside from delivery,has some genetic basis Risk is reduced by high levels of paternal antigens, via sexual contact Most common of dangerous pregnancy complications, found in about 10% of pregnancies, usually in 3rd trimester; esp. dangerous in developing countries (4) May cause premature birth, may develop into eclampsia, involving seizures, cardiac arrest, cerebral hemorrhage, death; fetus has higher risk of prematurity, stillbirth, growth restriction - may force choice between survival of baby vs. mother Usually considered as just a maladaptive side effect of pregnancy Haig (1993, 2007) provides evidence that pre-eclampsia is due to placenta releasing factors that damage maternal epithelia, leading to increased blood pressure and flow to placenta Seen as high-risk strategy activated in minority of pregnancies in which there are inadequate nutrients for fetus, due to poor placental invasion and remodelling of spiral arteries, caused by various factors, including immunological resistance
First invasion (start of pregnancy): implantation deep in uterine tissue fails? early miscarriage Second invasion (end of 1st trimester): formation of placenta itself fails to reach completion (including inadequate modification of spiral arteries)? -> pre-eclampsia risk
Pre-eclampsia is primarily a disease of first pregnancies, and pregnancies after a change in sexual partner One study, 11.9% primigravidae, 4.7% same-paternity multigravidae, 24% new-paternity multigravidae (2) Longer sexual cohabitation reduces risk of pre-eclampsia: 40-45% with under 4 months, 5% for over 12 months in one study (3) More frequent intercourse, oral sex, reduces risk (4) Donor-insemination, donor-embryo pregnancies show higher risk Effects mediated by immunological interactions of paternal factors in semen, sperm, with female tissues, especially uterus During all human history, pre-eclampsia was involved in about 10% of births - was a significant morbidity and mortality factor IMPLICATIONS for evolution of human mating system and fertility?
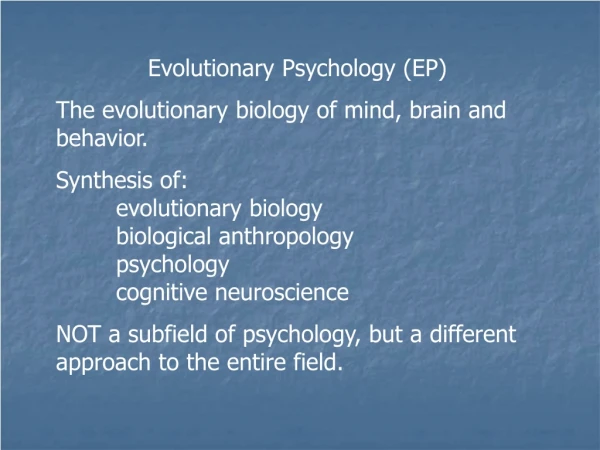
Humans exhibit very low fertility compared to other mammals -> Maximum fecundity (probability of conception in one cycle under ideal circumstances) is about 30% -> (despite what your mother may have told you) Most matings have a very low chance of producing a conception -> Ovulation is well-‘concealed’ in humans Macklon et al. 2002
And only about 30% of conceptions result in a live birth Macklon et al. 2002
Why is human fertility so low? (Robillard et al. 2002) Eclampsia appears restricted to humans Deep 2nd wave of placental invasion unique to humans, suggest is consequence of extended fetal nutritional needs in humans, especially the cost of brain growth ->in 2nd and 3rd trimester, human fetal brain requires about 60% of total fetal nutritional needs (vs about 20% in other mammals) Given role of cohabitation, frequent sex in reducing pre-eclampsia risk, expect selection for reduced fertility High fertility is better for higher fecundity, but increases pre-eclampsia risk-> simple graphical model Evolution of lower fertility may have involved selection for concealed ovulation in humans, as well as partner fidelity Might also expect sexual conflict over fertility? ALL OF THIS NEEDS TESTING!
morbidity and mortality of baby and mom go up with higher/faster fertility, due to pre-eclampsia risk fecundity goes up with fertility; have more babies sooner high low PE risk Fecundity high low low fertility high fertility Trade-off between fecundity and survival/morbidity: implications for human infertility and fertility in modern populations?
Evidence that high maternal blood pressure, if not pre-eclampsia, helps fetus -> High maternal blood pressure is associated with high baby birth weights, in several studies Evidence for the conflict model from genetic factors involved in pre-eclampsia Only one animal model for pre-eclampsia, which recapitulates all major human symptoms: p57kip2 knockout mice. p57kip2 is a maternally-expressed imprinted gene, that serves as a ‘master regulator’ of growth in pregnancy (2) In genome scan for pre-eclampsia, have found risk loci at 10q22 and 2p12 with strong parent of origin effects, and known imprinted genes in these regions These imprinted genes may influence pre-eclampsia risk indirectly via impaired placental development, OR directly via effects on placental factors that increase maternal blood pressure (3) Some fathers exhibit high risk (father one, 2x as likely to father another)
Implications of viewing pre-eclampsia as fetal ‘best of as bad job’ adaptation If pre-eclampsia is caused by release of placental factors, then there may be multiple factors with multiple targets Mothers should have developed counter-measures to limit the fetal manipulation Fetal actions must be distinguished from maternal responses: both may be interpreted as causes of pre-eclampsia (analogy with fever) Both hyper-activated in pre-eclampsia -> medical interventions that limit fetal effects should help, interventions that limit maternal responses should make matters worse [analogy with fever] More generally, pre-eclampsia may be caused by multiple forms of disruption to maternal-fetal tugs-of-war regarding placental invasiveness and regulation of maternal blood pressure
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Invasion of the placenta • Maternal-fetal food fights (a) Glucose concentration (b) Blood supply BABY ‘WINS’ with mild gestational diabetes, mild hypertension Dysregulated? Morbidity and mortality of baby and mom WHEN DOES MOTHER ‘WIN’? baby nourished at maternal optimum, involves restrictions on baby’s food supply Dysregulated? IUGR, intrauterine growth restriction
IUGR, intrauterine growth restriction Defined in terms of low birth weight (<2500g) (2) Involves 6-10% of all neonates, high levels of morbidity, mortality (>10X) (3) May be symmetrical (baby small, normal proportions) or asymmetrical (body especially small relative to head - brain ‘spared’) (4) has many causes, genetic and environmental (5) has lifelong consequences for health, via ‘fetal programming’, especially hypertension, heart disease, type 2 diabetes
Known factors associated with IUGR Many cases are idiopathic
Many cases of IUGR are caused by chromosomal abnormalities such as uniparental disomies (two chromosomes from same parent) IUGR also involves altered expression of imprinted genes in the placenta, in cytologically-normal individuals
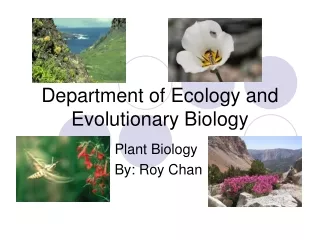
Silver-Russell syndrome involves severe IUGR IGF2-IGF2R (Haig & Graham 1991 Cell) (2) CDKN1C (Andrews et al. 2007 BMC Dev Biol) (3) GRB10 (Charalambous et al. 2003 PNAS) Beckwith- Wiedemann Syndrome Silver- Russell syndrome Mighty mouse Normal sized human
Evolutionary bases of fetal growth restriction? What are roles of maternal supply and fetal demand? Alternatives: (1) Poor environmental circumstances (nutrient limitation) (2) Maternal adaptations to constrain supply of nutrients to fetus dysregulated, due to genetic/environtmenal factors (3) Fetal adaptations to demand more nutrients become dysregulated, apparently as in pre-eclampsia Some evidence: -> fetal growth is partially-adjusted to maternal size by maternal factors (as shown via embryo transfer) -> first-born infants are smaller than 2nd or 3rd (about 200g), and adolescent females have smaller babies
Stages of Maternal-Offspring interactions (4) Gestation length Mother apparently have some control in early gestation (embryo screening) Offspring apparently controls parturition, in late gestation (placental hormones play role in inducing birth)(in sheep, fetus controls it) Offspring apparently ‘takes its time’ in good conditions, favors rapid delivery in poor conditions (infection, small-for-gestational-age deliver early) (d) Only single offspring can afford to take their time, what happens in litters? (in mammals, gestation length is negatively correlated with litter size)
Stages of Maternal-Offspring interactions • Conception, menstruation and early survival of the embryo • Invasion of the placenta • Maternal-fetal food fights (a) Glucose concentration (b) Blood supply • Gestation length • Survival of the fattest and cutest, or infanticide • Sucking, crying, weaning, whining • Survival and increased reproduction of the slower-developing child
Survival after birth Dramatic shift in power and control, from fetus to mother Opportunity for mother to choose whether or not to raise child (3) Infanticide, and infant exposure, have been common in human history, usually by the mother, commonly a mother in a bad situation (young, poor) COSTS AND BENEFITS TO MATERNAL AND FETAL GENES, of infanticide? Mother COST: energetics, time of 9-month gestation (& social costs?) BENEFIT: avoid raising low-fitness offspring, any in bad situation -> selects for maternal ‘screening’ of neonate quality/vigor (2) Fetus COST: death BENEFIT: inclusive fitness benefit, to mother, of not raising very low-fitness offspring -> selects for mechanisms that convince mother of high value of baby
Survival of the fattest Human fetuses spend last several weeks of pregnancy depositing fat, rather than growing in skeletal size -baby growth strategy: (a) survive if premature, then,(b) stockpile nutrients as fat -fat is most variable component of size, 46% of variance in one study; accounted for 70% of baby weight reduction in mothers who exercised intensely WHY SO FAT? (a) thermal insulation? not supported (b) honest signal to mother of high value? - ‘baby fat’ a post-natal equivalent of hCG - is deposited where can be seen - mothers select for fat babies (c) baby fat has high early survival value, fuels rapid brain growth (d) heavy, fat babies suffer less disease, live longer
Implications of baby fatness for evolution of health and disease Key role of long-chain fatty acids (eg DHA, AA) in fetal and infant development, and perhaps human origins (2) Apparent existence of placental mechanisms for acquiring long-chain fatty acids - what genes involved? positively selected in human lineage? subject to maladaptive mutation in fetal growth restriction? local adaptation? (3) Is there maternal-fetal conflict over fatty acids, as for blood and glucose? In late gestation, fetus takes fatty acids direct from mother’s brain - may contribute to post-partum depression or psychosis.
ANOTHER CASE, NOT DISCUSSED FURTHER • Gestational anemia: • Iron is food for bacteria • Iron is necessary for blood clotting • Mother iron level is set to balance risk of bacterial infections against risk of blood loss • Fetuses ‘want’ (selected for) iron levels to minimize bacterial infections but do not incur costs due to blood loss • Mother’s blood does not clot as well and is more prone to blood loss during birth and from injuries. • Fetus is less prone to bacterial infections