Download
1 / 9
90 likes | 543 Vues
Estimation of ‘Burn % Total Body Surface Area (TBSA)’ and fluid resuscitation. JAHD – 1/5/2012 Peter Cottrell. E xposure. TBSA Burn % = an assessment measure of burns of the skin. Two different methods are used depending on the age/size of the human: Adults - the Wallace “Rule of Nines”

E N D
Estimation of ‘Burn % Total Body Surface Area (TBSA)’ and fluid resuscitation JAHD – 1/5/2012 Peter Cottrell
Exposure TBSA Burn % = an assessment measure of burns of the skin. Two different methods are used depending on the age/size of the human: • Adults - the Wallace “Rule of Nines” • Children - the ‘Lund-Browder chart’ (can be used in adults) These methods assesses the percentage of burns and are used to help guide treatment (e.g. fluid resuscitation) and become part of the guidelines to determine transfer to a burn unit.
Assessing the burned area • It is important that all of the burn is exposed and assessed. • During assessment, the environment should be kept warm, and small segments of skin exposed sequentially to reduce heat loss. • Pigmented skin can be difficult to assess, and in such cases it may be necessary to remove all the loose epidermal layers to calculate burn size.
“Rule of Nines” (1) • The body is divided into anatomical regions that represent 9% of the total body surface. • The outstretched palm and fingers approximates to 1% of the body surface area. If the burned area is small, assess how many times your hand covers the area. • Morbidity and mortality rises with increasing burned surface area. It also rises with increasing age so that even small burns may be fatal in elderly people.
“Rule of Nines” (2) • Head = 9% • Chest (front) = 9% • Abdomen (front) = 9% • Upper/mid/low back and buttocks = 18% • Each arm = 9% (front = 4.5%, back = 4.5%) • Genitals/Perineum = 1% • Each leg = 18% (front = 9%, back = 9%)
‘Lund-Browder Chart’ This chart, if used correctly, is the most accurate method. It compensates for the variation in body shape with age and therefore can give an accurate assessment of burns area in children. DON’T include areas of simple erythema!
Burn criteria requiring hospitalization • Greater than 15% burns in an adult • Greater than 10% burns in a child • Any burn in the very young, the elderly or the infirm • Any full thickness burn • Burns of special regions: face, hands, feet, perineum • Circumferential burns • Inhalation injury • Associated trauma or significant pre-burn illness: e.g. diabetes
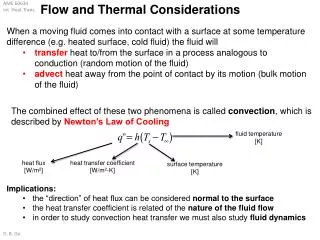
Fluid resuscitation – What to do? Fluid resus should be instituted as soon as possible. The volume of fluid infused depends upon the %BSA, time passed since injury and patients weight. In the first 24 hours: Parklands: Crystalloid resuscitation with Hartmanns 24 hour fluid requirement = 4 x %BSA x Wt (Kg) Give half over the first 8 hours, and the remainder over the next 16-24 hrs Following this, fluid is titrated based upon urine output and observations at intervals of four to six hours (i.e. packed cell volume, plasma sodium, base excess, and lactate).
Fluid resuscitation – Important points • The least amount of fluid necessary to maintain adequate organ perfusion should be given • The volume infused should be continually titrated to avoid both under- and over-resuscitation Resuscitation should be continuously assessed and adjusted according to urine output, pulse, blood pressure, capillary return, consciousness, haematocrit and respiratory rate.