Hyponatremia
Hyponatremia. By James Yost, MD, MS, MBA Emory Family Medicine. Hyponatremia. Definition Epidemiology Physiology Pathophysiology Types Clinical Manifestations Diagnosis Treatment. Hyponatremia. Definition: Commonly defined as a serum sodium concentration 135 meq/L

Hyponatremia
E N D
Presentation Transcript
Hyponatremia By James Yost, MD, MS, MBA Emory Family Medicine
Hyponatremia • Definition • Epidemiology • Physiology • Pathophysiology • Types • Clinical Manifestations • Diagnosis • Treatment
Hyponatremia • Definition: • Commonly defined as a serum sodium concentration 135 meq/L • Hyponatremia represents a relative excess of water in relation to sodium.
Hyponatremia • Epidemiology: • Frequency • Hyponatremia is the most common electrolyte disorder • incidence of approximately 1% • prevalence of approximately 2.5% • surgical ward, approximately 4.4% • 30% of patients treated in the intensive care unit ocw.jhsph.edu
Hyponatremia • Epidemiology Cont. • Mortality/Morbidity • Acute hyponatremia (developing over 48 h or less) are subject to more severe degrees of cerebral edema • sodium level is less than 105 mEq/L, the mortality is over 50% • Chronic hyponatremia (developing over more than 48 h) experience milder degrees of cerebral edema • Brainstem herniation has not been observed in patients with chronic hyponatremia
Hyponatremia • Epidemiology Cont. • Age • Infants • fed tap water in an effort to treat symptoms of gastroenteritis • Infants fed dilute formula in attempt to ration • Elderly patients with diminished sense of thirst, especially when physical infirmity limits independent access to food and drink
Hyponatremia • Physiology • Serum sodium concentration regulation: • stimulation of thirst • secretion of ADH • feedback mechanisms of the renin-angiotensin-aldosterone system • renal handling of filtered sodium www.daviddarling.info
Hyponatremia • PhysiologyCont. • Stimulation of thirst • Osmolality increases • Main driving force • Only requires an increase of 2% - 3% • Blood volume or pressure is reduced • Requires a decrease of 10% - 15% • Thirst center is located in the anteriolateral center of the hypothalamus • Respond to NaCL and angiotensin II
Hyponatremia • PhysiologyCont. • Secretion of ADH • Synthesized by the neuroendocrine cells in the supraoptic and paraventricular nuclei of the hypothalamus • Triggeres: • Osmolality of body fluids • A change of about 1% • Volume and pressure of the vascular system • Increases the permeability of the collecting duct to water and urea
Hyponatremia • PhysiologyCont • renin-angiotensin-aldosterone • Renin • Stemuli are perfusion pressure, sympathetic activity, and NaCl delivery to the macula densa • Increase in NaCl delivery to the macula decreases the GFR by decrease in the renin secretion • Aldosterone • Reduces NaCl excretion by stimulating it’s resorption • Ascending loop of Henle • Distal tubule • Collecting duct
Hyponatremia www.merricks.com/tech_electrolyte_new.htm
Hyponatremia • PhysiologyCont. • extracellular-fluid and intracellular-fluid compartments make up 40 percent and 60 percent of total body water • renal handling of water is sufficient to excrete as much as 15-20 L of free water per day • sodium is the predominant osmole in the extracellular fluid (ECF) compartment and serum
Hyponatremia • Pathophysiology • hyponatremia can only occur when some condition impairs normal free water excretion • acute drop in the serum osmolality: • neuronal cell swelling occurs due to the water shift from the extracellular space to the intracellular space • Swelling of the brain cells elicits 2 responses for osmoregulation, as follows: • It inhibits ADH secretion and hypothalamic thirst center • immediate cellular adaptation
Hyponatremia • Types • Hypovolemic hyponatremia • Euvolemic hyponatremia • Hypervolemic hyponatremia • Redistributive hyponatremia • Pseudohyponatremia
Hypovolemic hyponatremia • develops as sodium and free water are lost and/or replaced by inappropriately hypotonic fluids • Sodium can be lost through renal or non-renal routes www.grouptrails.com/.../0-Beat-Dehydration.jpg
Hypovolemic hyponatremia • Nonrenal loss • GI losses • Vomiting, Diarrhea, fistulas, pancreatitis • Excessive sweating • Third spacing of fluids • ascites, peritonitis, pancreatitis, and burns • Cerebral salt-wasting syndrome • traumatic brain injury, aneurysmal subarachnoid hemorrhage, and intracranial surgery • Must distinguish from SIADH www.jupiterimages.com
Hypovolemic hyponatremia • Renal Loss • Acute or chronic renal insufficiency • Diuretics www.ct-angiogram.com/images/renalCTangiogram2.jpg
Euvolemic hyponatremia • Normal sodium stores and a total body excess of free water • Psychogenic polydipsia, often in psychiatric patients • Administration of hypotonic intravenous or irrigation fluids in the immediate postoperative period
Euvolemic hyponatremia • administration of hypotonic maintenance intravenous fluids • Infants who may have been given inappropriate amounts of free water • bowel preparation before colonoscopy or colorectal surgery
Euvolemic hyponatremia • SIADH • downward resetting of the osmostat • Pulmonary Disease • Small cell, pneumonia, TB, sarcoidosis • Cerebral Diseases • CVA, Temporal arteritis, meningitis, encephalitis • Medications • SSRI, Antipsychotics, Opiates, Depakote, Tegratol
Hypervolemic hyponatremia • Total body sodium increases, and TBW increases to a greater extent. • Can be renal or non-renal • acute or chronic renal failure • dysfunctional kidneys are unable to excrete the ingested sodium load • cirrhosis, congestive heart failure, or nephrotic syndrome
Redistributive hyponatremia • Water shifts from the intracellular to the extracellular compartment, with a resultant dilution of sodium. The TBW and total body sodium are unchanged. • This condition occurs with hyperglycemia • Administration of mannitol
Hyponatremia • Pseudohyponatremia • The aqueous phase is diluted by excessive proteins or lipids. The TBW and total body sodium are unchanged. • hypertriglyceridemia • multiple myeloma
Hyponatremia • Clinical Manifestations • most patients with a serum sodium concentrationexceeding 125 mEq/L are asymptomatic • Patients with acutely developing hyponatremia are typically symptomatic at a level of approximately 120 mEq/L • Most abnormal findings on physical examination are characteristically neurologic in origin • patients may exhibit signs of hypovolemia or hypervolemia
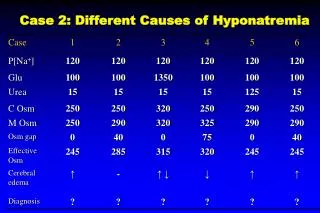
Hyponatremia • Diagnosis • CT head, EKG, CXR if symptomatic • Repeat Na level • Correct for hyperglycemia • Laboratory tests provide important initial information in the differential diagnosis of hyponatremia • Plasma osmolality • Urine osmolality • Urine sodium concentration • Uric acid level • FeNa
Hyponatremia • Laboratory tests Cont. • Plasma osmolality • normally ranges from 275 to 290 mosmol/kg • If >290 mosmol/kg : • Hyperglycemia or administration of mannitol • If 275 – 290 mosmol/kg : • hyperlipidemia or hyperproteinemia • If <275 mosmol/kg : • Eval volume status
Hyponatremia • Laboratory tests Cont. • Plasma osmolality < 275 mosmol/kg • Increased volume: • CHF, cirrhosis, nephrotic syndrome • Euvolemic • SIADH, hypothyroidism, psychogenic polydipsia, beer potomania, postoperative states • Decreased volume • GI loss, skin, 3rd spacing, diuretics
Hyponatremia • Laboratory tests Cont. • Urine osmolality • Normal value is > 100 mosmol/kg • Normal to high: • Hyperlipidemia, hyperproteinemia, hyperglycemia, SIADH • < 100 mosmol/kg • hypoosmolar hyponatremia • Excessive sweating • Burns • Vomiting • Diarrhea • Urinary loss
Hyponatremia • Laboratory tests Cont. • Urine Sodium • >20 mEq/L • SIADH, diuretics • <20 mEq/L • cirrhosis, nephrosis, congestive heart failure, GI loss, skin, 3rd spacing, psychogenic polydipsya • Uric Acid Level • < 4 mg/dl consider SIADH • FeNa • Help to determine pre-renal from renal causes
Hyponatremia • Treatment • four issues must be addressed • Asyptomatic vs. symptomatic • acute (within 48 hours) • chronic (>48 hours) • Volume status • 1st step is to calculate the total body water • total body water (TBW) = 0.6 × body weight
Hyponatremia • Treatment Cont. • next decide what our desired correction rate should be • Symptomatic • immediate increase in serum Na level by 8 to 10 meq/L in 4 to 6 hours with hypertonic saline is recommended • acute hyponatremia • more rapid correction may be possible • 8 to 10 meq/L in 4 to 8 hours • chronic hyponatremia • slower rates of correction • 12 meq/L in 24 hours
Hyponatremia • Symptomatic or Acute • Treatment Cont. - Here comes the Math!!! • estimate SNa change on the basis of the amount of Na in the infusate • ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1) • ΔSNa is a change in SNa • [Na + K]inf is infusate Na and K concentration in 1 liter of solution • OH MY GOD, what did he just say!!!!!!!!!!!!!!!!!!
Hyponatremia • IV Fluids • One liter of Lactated Ringer's Solution contains: • 130 mEq of sodium ion = 130 mmol/L • 109 mEq of chloride ion = 109 mmol/L • 28 mEq of lactate = 28 mmol/L • 4 mEq of potassium ion = 4 mmol/L • 3 mEq of calcium ion = 1.5 mmol/L • One liter of Normal Saline contains: • 154 mEq/L of Na+ and Cl− • One liter of 3% saline contains: • 514 mEq/L of Na+ and Cl−
Hyponatremia • Example: • a 60 kg women with a plasma sodium of 110 meq/L • Formula: • ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1) • What is the TBW? • How high will 1 liter of normal saline raise the plasma sodium? • Answer: • TBW is 30 L • Serum sodium will increase by approximately 1.4 meq/L for a total SNa of 111.4 meq/L
Hyponatremia • Example: • a 90 kg man with a plasma sodium of 110 meq/L • Formula: • ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1) • What is the TBW? • How high will 1 liter of 3% saline raise the plasma sodium? • Answer: • TBW is 54 L • Serum sodium will increase by approximately 7.3 meq/L for a total SNa of 117.3 meq/L
Hyponatremia • Asymptomatic or Chronic • SIADH • response to isotonic saline is different in the SIADH • In hypovolemia both the sodium and water are retained • sodium handling is intact in SIADH • administered sodium will be excreted in the urine, while some of the water may be retained • possible worsening the hyponatremia
Hyponatremia • Asypmtomatic or Chronic • SIADH • Water restriction • 0.5-1 liter/day • Salt tablets • Demeclocycline • Inhibits the effects of ADH • Onset of action may require up to one week
Hyponatremia • Example: • 85 y/o male with weakness and head ache • SNa is 118 mEq/L • Plasma osmolality is 254 mosmol/kg • Urine osmolality is 130 mosmol/kg • Urine sodium >20 mEq/L • Uric acid is 3mg/dl • What type of hyponatremia does this patient have? • What additional labs/studies would you want?
Ouch!!!!! Hyponatremia • Example Cont.: • Noncontrast CT Head: • Tx • Call Neurology and neurosurgery • Free water restriction trismus1.wordpress.com
Hyponatremia • Example: • 63 y/o female at 75 Kg with N/V/D for 4 days • SNa is 108 mEq/L • She has had one seizure in the ambulance • Plasma osmolality is 251 mosmol/kg • Urine osmolality is 47 mosmol/kg • Uric acid is 6mg/dl • What type of hyponatremia does this patient have? • What additional labs/studies would you want? hollywoodphony.files.wordpress.com
Hyponatremia • How will you Tx her? • Calculate the total body water • 0.5 x weight = 37.5 L • What rate of correction do you want? • 8 to 10 mEq/L in 6 to 8 hours • What fluid will you use? • 3% Saline • How will you calculate the amount of sodium to give her? • ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1) • How will her sodium increase after 1 liter of 3% saline? • By 10.8 mEq/L to 118.8 mEq/L
Hyponatremia • What other medication will she need? • Lasix and a foley • Her sodium increases to 118.8 mEq/L over the next 8-10 hours. How will you continue to correct her hyponatremia? • ΔSNa = {[Na + K]inf − SNa} ÷ (TBW + 1) • ΔSNa = 154mEq/L – 118.8mEq/L ÷ 38.5L = 0.9 mEq/L • So 2 liters of normal saline over the next 14 hours
Hyponatremia • Congrats!!!!!!!! You saved her! • Questions????