Download
1 / 28
280 likes | 392 Vues
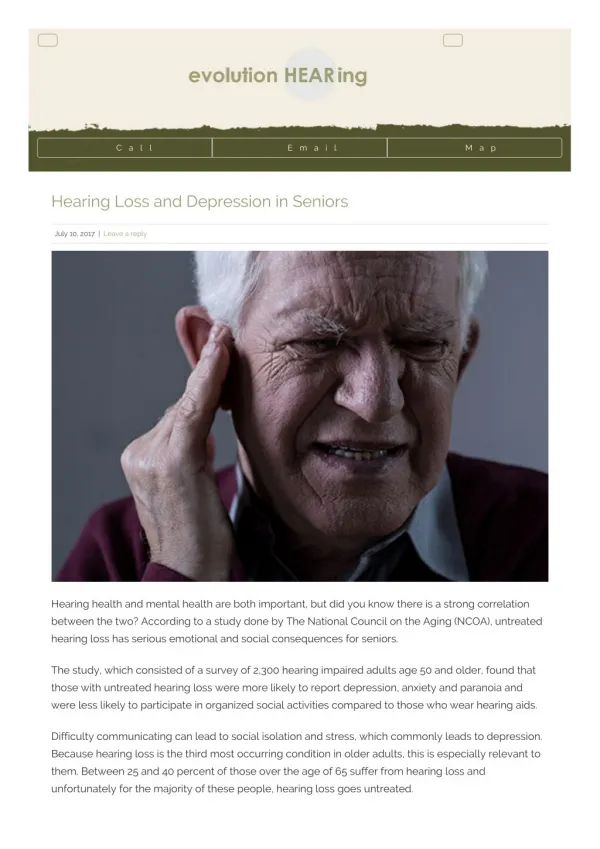
The Assessment Program for Seniors addresses depression in older adults, emphasizing that depressive disorders are not a normal part of aging. While temporary sadness is expected, persistent depression significantly impacts daily functioning. The prevalence of depression among seniors varies—from 1-5% in the general community to as high as 65% in nursing homes. This program outlines common mood disorders, symptoms, and risk factors, advocating for proper assessment and interventional strategies tailored to enhance wellness, social support, and mental health treatment.

E N D
Depression Assessment Program for Seniors Catherine R. Johnson, PsyD LP Associated Clinic of Psychology 2013 Minnesota Age & Disabilities Odyssey June 17, 2013
Mood Disorders Depressive disorder is not a normal part of aging. Emotional experiences of sadness, grief, response to loss, and temporary “blue” moods are normal. Persistent depression that interferes significantly with ability to function is not.
Prevalence of Depression: Age 65 and Older • 1-5% Community older adults • 13.5% Requiring home healthcare • 11.5% Hospitalized • 65% Nursing home have mental-health issues • Major depression – 12%-22% • Depressive symptoms – 17%-30% 5 Million with depressive symptoms
Suicide: General Population 11% 14.3 % of all suicides are age 65 or older White male age 85 and older –highest rate 75% had visited a doctor within the last month
Suicide: General Population 11% For every 100,000 people age 65 and older in each of the ethnic/racial groups below, the following number died by suicide in 2007: Non-Hispanic Whites — 13.5 per 100,000 Am Indian and Alaskan – 14.3 per 100,000 Asian and Pacific Islanders — 6.2 per 100,000 Hispanics — 6.0 per 100,000 Non-Hispanic Blacks — 5.1 per 100,000
Common Types of Mood Disorder or Related Disorder • Major Depression • Dysthymic • Cyclothymic • Bipolar I • Manic/Major Depression • Bipolar II • Hypomanic/ Major Depression • Other Disorders • Adjustment Disorder • Pseudodementia • Bereavement • Mood Disorder due to Medical Condition
Symptoms of Depression • Depressed or sad mood/irritable mood/agitated • Loss of interest in activities • Fatigue or loss of energy -Sleep Disorder • Psychomotor retardation –slow moving • Weight change • Difficulty concentrating and/or memory • Feelings of worthlessness/guilt • Thoughts of death of dying
More physical symptoms -pain More cognitive symptoms Hypersomnia Anorexia Less crying/mood disturbances Sense of personal helplessness Apathy Sense of emptiness/loss Irritability/hostility Withdrawal from activities Depression in older adults
Depression in older adults 50% personality disorder traits Physical illness; excess disability Institutionalization Loneliness
Risk Factors – Medical Illness • Comorbidity with medical illness • Metabolic: Hypothyroidism, Diabetes • Neurologic: Dementias, MS, Parkinson’s • Stroke, cancer • Rheumatoid Arthritis • Congestive heart failure and heart attack • Infections, Vitamin B 12 deficiency • Pain
Risk Factors – Medications • Psychotropic Medications • Antiparkinsonian agents • Anticancer drugs • Hormonal preparations • Antihypertensives • Pain medications • Alcohol
Risk Factors • Female • Unmarried and/or widowed • Recent bereavement • Stressful live event • Lack of supportive social network • caregiver • Satisfaction with supportive services • Perceived empathy • Physical problems/pain • Education HS • Impaired functioning • Heavy alcohol use
Risk Factors • Demographic; age, sex, race, ethnicity • Early Life; education, childhood traumas • Late Life; occupation, income, marital status • Current Event; coping style and strategies • Social Integration; religious affiliation, voluntary activities, neighborhood stability • Vulnerability; chronic stressor, social support, isolation
Challenges of Recognition of and Treatment of Depression • Often undiagnosed or misdiagnosed • Historical development of care which focus on the medical model of care • Insufficient mental-health services • Environment exacerbates • Comorbidity with medical illness • Cultural ageism/gerophobia/internalized ageism • Older adults attitudes about aging and death • Insufficient research
Untreated Depression • Increase decline in function • Increase disability and worsen symptoms • Complicates the course of dementia • Complicates nursing/medical care: higher use of health care system • Increase costs • Diminishes quality of life for the family • Increase mortality
Identify risk factors Assess at-risk person with GDS-SF or PHQ-9 Note symptoms/onset severity/duration Review medical record/history Check for depressogenic meds Check for systematic and metabolic processes Assess cognitive function – SLUMs Assess functional disability - ACL Assessment Parameters
If severe (GDS-SF 11 or higher) and 5-9 symptoms: Refer for psychiatric evaluation Treatment options: anti-depressant meds and/or psychotherapy, hospitalization, ECT If mild to moderate (GDS-SF 6-10) and <5 symptoms: refer for mental-health evaluation For all persons develop interdisciplinary individual plan, document, and monitor Care Parameter
Safe precaution Remove/control depressogenic meds Correct metabolic disturbance/pain Promote wellness (nutrition, sleep, physical exercise) Enhance physical function –ACL test Enhance social support Maximize autonomy Encourage relaxation and engagement in pleasant activities Problem solve Care Plan Content
Provide information about physical/mental health illness Stress the importance of adherence to prescribed regimen Ensure mental health community linkup Track info/outcome Provide information to service provides to coordinate care Educate caregivers to continue efforts Education/Cord. all parties involved. Care Plan Content/Follow -Up
Cognitive Behavioral Cognitive/Behavioral Therapy Brief psychodynamic Life review Reminiscence Problem Solving Interpersonal Therapy Effective Psychotherapies
Antidepressant Medication • Most frequently prescribed to treat depression • Valuable when properly regulated and scrupulously supervised • Have consider side effects which limit use
Preferred Treatment • Preferred treatment for older adults residing is a combination of antidepressant medication and psychotherapy. However, for those who cannot tolerate medication, psychotherapy is the primary treatment alternative.
Advancing Mental-Health Services • Health care providers can mitigate depression experienced by older adults. • Employee mental-health training is available and effective to mitigate depression if a formal program is put in place.
Advancing Mental-Health Services • The Geriatric Depression Scale can be administered by health-care providers and is an effective at screening (vs. diagnosing) for depression in older adults with mild-to- moderate cognitive impairment. • PHQ-9
Personal Impact • Studies show that when persons trained to interact empathically with older adults visited older adult 2 times per week for one hour, those older adults showed significant decreases in depression and greater life satisfaction.
Conclusion • Psychologist, health-care providers, training and psychological instruments, and the evaluation processes all contribute to an effective mental-health program for older adults. When pulled together in a systematic way, the mitigation of depression among this population is amenable to success.
Resources Senior LinkAge Line 1-800-333-2433 www.MinnesotaHelp.info Try This Series: www.ConsultGeriRN.org
The Depression Assessment Program for Seniors (DAPS) is a screening and intervention program for older adults based on the evidence based program Healthy IDEAS (Identifying Depression, Empowering Activities for Seniors). DAPS is supported, in part, by a CS/SD grant from the Minnesota Department of Human Services (DHS). Viewpoints and opinions in this presentation do not necessarily represent official DHS policy. If you would like more information about DAPS, contact: DAPS partners include: Jewish Family Service of St. Paul (project lead) Highland Block Nurse Program Ramsey County Human Services National Alliance on Mental Illness MN West 7th Community Center Optage, Inc.