Download
1 / 22
220 likes | 366 Vues
The HIV Engagement in Care Cascade. Edward Gardner, MD Associate Professor of Medicine Denver Public Health University of Colorado Denver. Test and Treat. Models made sense… But it seemed a lot needed to happen in between We were thinking more like

E N D
The HIV Engagement in Care Cascade Edward Gardner, MD Associate Professor of Medicine Denver Public Health University of Colorado Denver
Test and Treat Models made sense… But it seemed a lot needed to happen in between We were thinking more like Test and Link and Retain and Re-engage and Treat and Persist and Adhere and Re-engage …
HIV Care Continuum Adapted from Eldred et al AIDS Patient Care STDs 2007;21(Suppl1):S1-S2 Cheever LW Clin Infect Dis 2007;44:1500-2
Test and Treat for HIV Prevention Das M et al. PLoS One 2010;5:e11068
Treatment as Prevention – HPTN 052 HPTN-052 96% reduction In HIV incidence NEJM 2011;365: 493-505.
CDC Cascade MMWR December 2, 2011 / 60(47);1618-1623
Review Search Strategy • PubMed search - cross-match of HIV or AIDS with • Prevalence United States • Incidence United States • Late diagnosis • Linkage to care • Retention in care • Engagement in care • Adherence • Persistence • Resistance • Bibliographies of pertinent articles were reviewed • Emphasis was based on population based studies over cohort or single institution studies
Linkage to HIV Care • Original Cascade estimated about 75% linkage • Marks et al.1 meta-analysis found 72% linkage in studies after 2003 • MMWR2 estimated 77% linkage • Dombrowski et al.3 showed 88% linkage in 3 months in Seattle/King County Washington • Denver Public Health Data (unpublished): • Final Estimate: 72 – 88% 1AIDS 2010, 24:2665–2678, 2MMWR 2011 / 60(47);1618-1623, 3AIDS 2012, 26:77-86.
Retention in HIV Care • Original Cascade estimated 50% retention • Marks et al.1 meta-analysis – 59% retention • MMWR2 – 51% • Torian et al.3, New York City – 46% (regular care) • Hall et al.4, 13 U.S. areas – 59% (1 visit/year) • Tripathi et al.5, South Carolina – 50% • Dombrowski et al.6, Seattle – 66% • Final Estimate: 46 – 66% 1AIDS 2010, 24:2665–2678, 2MMWR 2011 / 60(47);1618-1623, 3AIDS Pt Care STDs 2011;25:79-88, 4JAIDS 2012;60:77-82, 5AIDS Res Hum Retrovir 2011;27:751-58, 6AIDS 2012, 26:77-86.
Attainment of an Undetectable Viral Load • Original Cascade estimated 60% undetectable • Marks et al.1: 62% < 75 cps/ml, 73% < 400 cps/ml • MMWR2: 77% • Hall et al.3: 73% • Dombrowski et al.4: 65% • InCare Campaign5: 70% • Final Estimate: 62 – 77% 1AIDS 2010, 24:2665–2678, 2MMWR 2011 / 60(47);1618-1623, 3AIDS Pt Care STDs 2011;25:79-88, 4AIDS 2012, 26:77-86, 5www.incarecampaign.org
Simulations of the Engagement in HIV Care Spectrum to Account for Inaccuracy in our Engagement Estimates
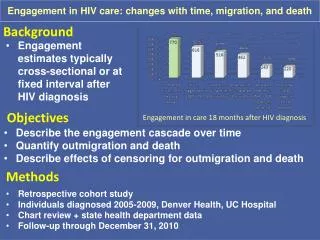
Denver Cascade over Time IAS 2012 Poster MOPDC0305
Denver Cascade over Time Censoring Out-Migration and Death IAS 2012 Poster MOPDC0305
Limitations • Different definitions of linkage and retention in different studies • Overlap in the stages of engagement in HIV care • Cross-sectional depiction of a longitudinal process • The review applies to the U.S. and not to resource-poor settings • Unable to assess the impact of financial barriers to HIV care in the U.S.
Conclusions • Engagement in care is critical to the successful management of HIV infection • For the individual • For the population • Deficiencies in the spectrum of engagement in care present formidable barriers to HIV care and ‘test and treat’ for HIV prevention: • Failure to diagnose • Failure to link to care • Failure to be retained in care • Failure to receive and adhere to antiretroviral therapy • Research is needed on ways to improve transitions across all steps in the engagement in care cascade
Comments • Universal Treatment is the “Treat” of Test & Treat • Data quality on engagement steps is improving • Engagement in Care research in HIV is likely applicable to other chronic illnesses • Cascade formats could be standardized and used worldwide as a snapshot of HIV Care
Thank YouTalk Supported by AIDS United Questions?