NaProTechnology Natural Procreative Technology
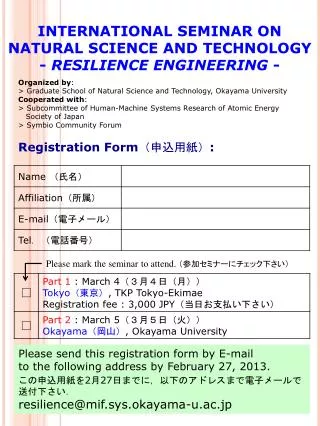
NaProTechnology Natural Procreative Technology. A multifactorial approach to the chronic problem of Infertility Dr. Phil C. Boyle MICGP, MRCGP, CFCMC Galway Clinic, Ireland Prof. Joseph Stanford MD, University of Utah, USA. 03 June 2011. Outline. Abstract Summary 3 Case Presentations

NaProTechnology Natural Procreative Technology
E N D
Presentation Transcript
NaProTechnology Natural Procreative Technology A multifactorial approach to the chronic problem of Infertility Dr. Phil C. Boyle MICGP, MRCGP, CFCMC Galway Clinic, Ireland Prof. Joseph Stanford MD, University of Utah, USA 03 June 2011
Outline • Abstract Summary • 3 Case Presentations • Discussion points
Illness can be …… Acute Chronic Sudden onset Shorter duration May resolve spontaneously Tend to have single or few causes May be cured by single intervention or treatment Gradual onset Longer duration Rarely resolve spontaneously Usually have multiple causes Outcomes improved with multiple sustained interventions
Health conditions Acute Chronic Appendicitis Respiratory viral infection Fractured bone Asthma Diabetes Degenerative arthritis
Infertility Gradual, unknown, or early onset Ongoing issues Potential for recurrence Syndrome, not diagnosis Many possible causes Usually, more than one cause or factor present
Infertility Rarely completely “cured” by single intervention Can be treated with multiple interventions Rarely resolves spontaneously
Chronic vs Acute approach NaProTechnology ART Infertility indicates the presence of disease with the challenge to diagnose and treat for optimum health. Infertility presents a technical challenge to bypass the dysfunctional process.
Chronic vs Acute approach NaProTechnology ART Seeks to identify long-term health conditions and improve them over a reproductive lifetime Chronic perspective Long term health conditions are considered less important for short-term treatment. Acute perspective
Description Infertility is usually a consequence of multiple chronic conditions rather than a single acute condition. We propose that it is erroneous to apply acute medical interventions to a condition that is chronic in nature.
Low Hormones Low Endorphins Surgical Limited Mucus Infertility & Miscarriage Male Factor Diet & Nutrition Infection Adrenal Fatigue Immunological Others To be discovered
Possible Diagnoses from NaProTechnology Evaluation Hormonal Ultrasound Surgical Other *Although these diagnoses are hormonally mediated, at least in part, the diagnosis and management is not based on direct hormonal testing at this time. Fig. 3
Method Retrospective analysis of 3 case studies which demonstrate the multifactorial and chronic nature of infertility that were previously managed unsuccessfully with acute intervention using IVF (in Vitro Fertilisation) or ART (Assisted Reproductive Technology).
Results Demonstration of the multifactorial approach and 3 successful singleton live births using NPT (Natural Procreative Technology or NaProTechnology).
Conclusion Infertility can be treated successfully with a multifactorial approach which takes into account the chronic nature of infertility and targets treatment to manage multiple factors responsible for the condition.
Discussion Infertility is not a diagnosis but is often the expression of several underlying ill health conditions which if diagnosed and treated correctly will result in restoration of normal reproductive function.
Discussion - Continued Physicians ought to consider broader diagnostic possibilities in their evaluation of infertile couples. A multifactorial treatment strategy for the chronic condition of infertility may be more effective than the widespread acute strategy employed by ART.
Discussion - Continued Future studies looking at NPT and ART outcomes • Must be cohort studies and • Compare populations with similar patient characteristics
3 Case Presentations • Case A • Case B • Case C
Case A • Gravida 0 Para 0, • Female aged 41, Male aged 40, • Trying to conceive for 2 years, • Unexplained infertility, • 3 failed IUI and 2 failed IVF.
Case A • Presented for treatment – March 2009 • Unexplained Infertility • Lap and Dye – normal 2007 • Semen analysis – normal 2007 • IUI x 3 – FSH/LH and HCG - June 2008 • IVF x 2 • 3 Embryos transferred – Aug 2008 & March 2009
Case A – NPT Diagnoses • Chronic Endometritis • Progesterone deficiency • poor follicular function • & corpus luteum insufficiency • Hostile Cervical Mucus • Clinical endorphin deficiency • Mild food intolerance
Case A – NPT Treatments • Clinical endorphin deficiency • Naltrexone 2mg nocte • Mild food intolerance (IgG) • Egg yolk and soya www.camnutri.com
Case A – NPT treatment • Progesterone deficiency • poor follicular function • & corpus luteum insufficiency • Letrozole 2.5mg 10 tabs on day 3 • HCG 10,000 iu mid cycle • HCG 2,500 iu Peak +3,5,7
Case A – NPT Treatments • Hostile Cervical Mucus • Cabroceistine 375mg tid x 7 days, day 11 • Amoxycillin 500mg tid x 5 days, day 11 • PreSeed Vaginal Lubricant
Case A – NPT Treatments • Chronic Endometritis • Metronidazole 400mg BD x 3 weeks • Clarithromycin 500mg BD x 3 weeks • Pro biotic for 6 weeks Start day 14 of cycle
10 F 10 F H H H H Antibiotic treatment Positive Test!
Case A • 42 years old at conception. • Hormone support with cyclogest 400mg pv. twice daily until 8 weeks • Cyclogest 400mg pv nocte until 16 weeks gestation
Case A • She delivered a healthy baby boy by Caesarean section in November 2010, weighing 3180g.
Case A • CrMS Chart was critically important to the process • Timing of blood tests • Timing of HCG injections • Identify hostile mucus • Identify Brown Bleed – Chronic Endometritis
Case A IVF which attempted to solve the symptom of infertility through bypassing the natural process of conception was inappropriate and ineffective as she had several chronic conditions that needed to be treated in a targeted fashion to restore normal reproductive function
Case B • Gravida 1 Para 0 • Female aged 37 Male aged 39 • 7 years trying to conceive • Mildly polycystic ovaries and recurrent implantation failure • 3 failed IVF cycles, 3 fresh & 1 frozen transfer.
Case B • Presented on April 2009 • Trying to conceive since Jan 2002 • Cycle 32 to 25 days • Unplanned miscarriage at 11 weeks – 1999 • Diagnosis – Mild PCOD by ultrasound
Case B – Normal investigations • Laparoscopy ’01 &’08, • Hysteroscopy ‘09 • Semen analysis several tests – ’01- ’08 • Day 3 bloods • Thrombophillia Screen • Immunological testing “Chicago Bloods”
Case B – Treatments • Clomiphene • 50mg daily for 5 days, from day 3 of cycle x 4 • 100mg daily for 5 days, from day 3 of cycle x 4 • 150mg daily for 5 days, from day 3 of cycle x 4 • 12 cycles in total previously
Case B – Treatments • IVF x 3 stimulated cycles • Feb 2006 – March 2009 • Embryo transfer – 3 fresh and 1 frozen • 2 – 3 embryos each time • Additional Aspirin, Enoxaparin, Prednisolone 25mg with last IVF cycle despite normal testing
Case B – NPT Diagnoses • Progesterone deficiency – with corpus luteum insufficiency - Dramatic chart! • Polycystic Ovaries – with poor follicular function • Clinical endorphin deficiency • Clinical Adrenal fatigue
7 6 9 6 10F H 12 H H H H
Case B – NPT Treatments • Progesterone deficiency – with corpus luteum insufficiency - Dramatic chart! • Polycystic Ovaries – with poor follicular function • HCG 2,500iu P+3,5,7,9 • Letrozole 2.5mg – 16 tabs – day 3 • HCG 10,000 iu mid cycle
12 10F H H H H 14 10F H H H H 10F H H H H 17
Case B – NPT Treatments • Clinical endorphin deficiency • Naltrexone 3mg nocte • Clinical Adrenal fatigue • Hydrocortisone 5mg – 7am & 12 noon • Supplements • Vitamin D3 – 2,400iu daily • Omega 3 2000mg daily plus Folic acid
Case B – NPT Outcome • With treatment we achieved a normal appearing CrMS chart, with proven follicle rupture by ultrasound, and a healthy happy patient. • She conceived on her 5th cycle of treatment (second effective cycle) in April 2010
16F H H H H Positive Test!
Case B – NPT Pregnancy treatment • Cyclogest 400mg pv twice daily until 36 weeks gestation • Aspirin 75mg daily until 30 weeks • Prednisolone 25mg daily until 12 weeks
Case B – NPT Pregnancy Outcome • She had a normal vaginal delivery of a healthy baby boy, 3.130 Kg in January 2011 • Mother was 38 years old at delivery
16F H H H H Positive Test!
Case B – Comments • Immediately identified Corpus luteum insufficiency & confirmed restoration of normal function with treatment. • Patient’s well being improved with naltrexone and cortisol treatment. When this happens, we often find our treatment is more successful.
Case B – Comments • Although we did not feel aspirin or prednisolone were necessary we conceded to the patients request to give these medications as recommended by her previous doctor