ABDOMINAL HERNIAE
ABDOMINAL HERNIAE. A. WEISS M.D D.E.S , Chirurgie Générale,Viscérale et Laparoscopique A.F.S/A.F.S.A/DU - France References: Richard S.SNELL/ Clinical Anatomy/By SNELL/7e.Vol2 Seymour I. SCHWARTZ/ Principles of Surgery Companion Handbook/McGraw-Hill/1998

ABDOMINAL HERNIAE
E N D
Presentation Transcript
ABDOMINAL HERNIAE A. WEISS M.D D.E.S ,Chirurgie Générale,Viscéraleet Laparoscopique A.F.S/A.F.S.A/DU - France References: Richard S.SNELL/ Clinical Anatomy/By SNELL/7e.Vol2 Seymour I. SCHWARTZ/ Principles of Surgery Companion Handbook/McGraw-Hill/1998 F. C BRUNICARDI and others/Schwartz’s Principles of Surgery/McGraw-Hill/8e/2004.
DEFINITION: • A hernia is the protrusion of part of the abdominal contents beyond the normal confines of the abdominal wall . • It consists of three parts: the sac, the contents of the sac, and the coverings of the sac. • The hernial sac is a pouch ( diverticulum) of peritoneum and has a neck and a body. • The hernial contents may consist of any structure found within the abdominal cavity . • The hernial covering are formed from the layers of the abdominal wall throw which hernial sac passes.
It consists of three parts: the sac, the contents of the sac, and the coverings of the sac. A hernia is the protrusion of part of the abdominal contents beyond the normal confines of the abdominal wall .
TYPE OF ABDONINAL HERNIAE • Inguinal (indirect or direct). • Femoral. • Umbilical (congenital or acquired). • Epigastric (linea alba) . • Separation of the recti abdominis. • Incisional hernia. • Hernia of the linea semilunaris (Spigelian hernia). • Lumbar hernia ( Petit’s triangle hernia). • Internal hernia.
STRUCTURE OF THE ANTERIOR ABDOMINAL WALL : • Skin . • Superficial Fascia : • Superficial fatty layer (fascia of Camper ). • Deep membranous layer ( Scarpa’s Fascia ). • Deep fascia . • Muscles of the Anterior Abdominal Wall : • External Oblique . • Internal Oblique . • Transversus . • Rectus Abdominis . • Pyramidalis ( if present ). • Fascia Transversalis . • Extra Peritonial fat . • Parietal Peritoneum .
ANATOMY OF THE INGUINAL CANAL • The inguinal canal is an oblique passage through the lower part of the anterior abdominal wall and present an both sexes. • The canal is about 4 cm long in the adults and extends from the deep inguinal ring , a hole in the fascia transversalis , downward and medially to the superficial inguinal ring , a hole in the aponeurosis of the external oblique muscle . • It lies parallel to and immediately above the inguinal ligament . • In the newborn child, the deep ring lies almost directly posterior to the superficial ring so that the canal is considerably shorter at this age . • The DEEP INGUINAL RING : an oval opening in the fascia transversalis lies about 1.3 cm above the inguinal ligament midway between the anterior iliac spine and the symphysis pubis and related to it medially are the inferior epigastric vessels . • The SUPERFICIAL RING is a triangular-shaped defect in the aponeurosis of the external oblique muscle and lies immediately above and medial to the pubis tubercle .
ANATOMY OF THE INGUINAL CANAL • Walls of the INGUINAL CANAL : • Anterior wall : the aponeurosis of the External Oblique muscle . • Posterior wall : the Fascia Transversalis . • Inferior wall or Floor of the canal : the inguinal ligement ( rolled –under inferior edge of the aponeurosis of the External Oblique muscle ) . • Superior wall or the roof of the canal :The conjoint tendon ( arching lowest fibers of the Internal oblique and Transversus abdominis muscles ) .
ANATOMY OF THE INGUINAL CANAL • Contents of the INGUINAL CANAL : • Spermatic cord : • Vas deferens . • Testicular artery . • Testicular veins (pampinform plexus ). • Testicular lymph vessels . • Autonomic nerves . • Processus vaginalis ( remains of ) . • Cremasteric artery . • Artery of the vas deferens . • Genital branch of the genitofemoral nerve . • Other structures : • Ilio-hypogastric nerve . • Ilioi-nguinal nerve .
THE MYOPECTINEAL ORIFICE OF FRUCHAUD : • Fruchaud's contribution to inguinal herniology was to examine the common anatomic etiology of direct, indirect, and femoral hernias, rather than to look at each individually . • The termmyopectineal orifice, an area bound superiorly by the internal oblique and transversusabdominis muscles, medially by the rectus muscle and sheath, laterally by the iliopsoas muscle, and inferiorly by Cooper's ligament (pecten pubis). • Critical anatomic landmarks such as the inguinal ligament, spermatic cord, and the femoral vessels are contained within this area. This funnel-shaped orifice is lined in its entirety by the transversalis fascia. Fruchaud's concept is that the fundamental cause of all groin hernia is failure of the transversalis fascia to retain the peritoneum.
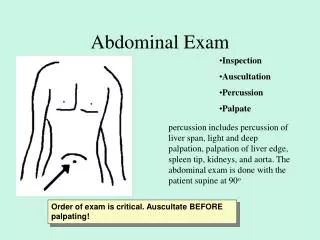
CLINICAL MANIFISTATIONS • The natural history of hernias is a slow enlargement to the point of irreducibility and disfigurement, with the risk of strangulation. • The discomforts produced by hernias are always worse at the end of the day and are relieved at night when the patient reclines and the hernia reduces. • Groin pain without a demonstrable hernia usually does not indicate the onset of a hernia. • Most hernias develop insidiously, but some are precipitated by a single forceful muscular event. • Typically, a hernial sac with its contents enlarges and transmits a palpable impulse when the patient strains or coughs. • Usually, the patient must stand during the examination because it is impossible to palpate a reduced groin hernia when the patient is supine. • Hydrocelestransilluminate, but hernias do not. • Hernias undetectable by physical examination can be demonstrated by using ultrasound or computed tomography (CT). • Strangulation produces intense pain in the hernia, followed quickly by tenderness, intestinal obstruction, and signs or symptoms of sepsis.
INDICATIONS FOR SURGERY • All hernias should be repaired unless local or systemic conditions of the patient preclude a safe outcome. • The possible exception is a hernia with a wide neck and shallow sac that is anticipated to enlarge slowly. • Trusses are helpful in the management of small hernias when operation is contraindicated. • Trusses are contraindicated for patients with femoral hernias.
HERNIAS OF THE GROIN ( Inguinal and femoral ) • ETIOLOGY: Intraperitoneal hypertension • Presumed Causes of Groin Herniation : • Coughing . • Chronic obstructive pulmonary disease. • Obesity . • Straining ( Constipation ,Prostatism). • Pregnancy. • Family history of a hernia • Ascites • Defective collagen synthesis • Previous right lower quadrant incision • Congenital connective tissue disorders • Cigarette smoking • Heavy lifting • Physical exertion (?)
HERNIAS OF THE GROINDIFFERENTIAL DIAGNOSIS • Lymphoma. • Retroperitoneal sarcoma. • Metastasis. • Testicular tumor. • Varicocele. • Epididymitis. • Testicular torsion. • Hydrocele. • Ectopic testicle. • Undescended testicle. • Femoral artery aneurysm or pseudoaneurysm. • Lymph node. • Sebaceous cyst. • Hidradenitis. • Cyst of the canal of Nuck (female). • Saphenous varix. • Psoas abscess. • Hematoma.
HERNIAS OF THE GROIN 1- Indirect inguinal hernia : The indirect inguinal hernia can be summarized as follow : • It is the remains of the processusvaginalis and therefore is congenital in origin. • It is more common than a direct inguinal hernia. • It is mutch more common in males than females. • It is more common on the right side. • The hernial sac enters the inguinal canal through the deep inguinal ring and lateral to the interior epigastricvessels,the neck of the sac is narrow. • The hernial sac may extend down into the scrotum or labium majus.
HERNIAS OF THE GROIN 2 - Direct inguinal hernia : The direct inguinal hernia can be summarized as follow : • It is common in old men with week abdominal muscles and is rare in women. • The hernial sac blugesforwradthrowgh the posterior wall of the inguinal canal medial to the inferior epigastric vessels. • The neck of the hernial sac is wide.
HERNIAS OF THE GROINPARTICULAR CASE Sliding Inguinal Hernia: It is defined as any hernia in which part of the sac is the wall of a viscus. It is rarely found in patients less than 30 years of age, but increases to 20% after the age of 70. On the right, the cecum, ascending colon, or appendix are most commonly involved, and on the left, the sigmoid colon is involved. The uterus, fallopian tube, ovary, ureter, and bladder can be involved on either side. The sliding component is usually found on the posterolateral side of the internal ring. it is not necessary to resect hernia sacs, and that simple reduction into the preperitoneal space is sufficient. This eliminates the primary danger associated with sliding hernias, which is injury to the viscus during high ligation and sac excision.
HERNIAS OF THE GROIN 3 - Femoral hernia : The femoral hernia can be summarized as follow : • A protrusion of abdominal parietal peritoneum down throwgh the femoral canal to from the hernial sac. • It is more common in women than in men . • The neck of the hernial sac lies below and lateral to the pubic tubercle. • The neck of the hernial sac lies at the femoral ring and at that point is related interiorly to the inguinal ligament, posterioly to the pectineal ligament, laterally to the femoral vien,and medially to the sharp free edge of the lacunar ligament.
HERNIAS OF THE GROININGUINAL HERNIA REPAIRS Open anterior ,Nonprosthetic: Marcy, Bassini, Moloney Darn, McVay Cooper's Ligament Repair, Shouldice. Open anterior ,Prosthetic : Lichtenstein Tension-Free Hernioplasty, Mesh Plug and Patch.
HERNIAS OF THE GROININGUINAL HERNIA REPAIRS • Open preperitoneal, Nonprosthetic. • Open preperitoneal, Prosthetic: Read-Rives, Wantz/Stoppa/Rives. • Combination anterior and preperitoneal, Prosthetic. • Laparoscopic inguinal herniorrhaphy.
HERNIAS OF THE GROIN Complications of Groin Hernia Repairs • Recurrence. • Chronic Groin Pain. • Hematoma. • Seroma. • Bladder Injury. • Wound Infection. • Osteitis Pubis • Prosthetic Complications • Ischemic orchitis. • Testicular atrophy. • Dysejaculation syndrome (rare). • Hydroceles. • Testicular descent. • Laparoscopic Complications.
UMBILICAL HERNIA • Umbilical hernias develop at the umbilical ring and may be present at birth or develop gradually during the life of the individual • Umbilical hernias are present in approximately 10% of all newborns and are more common in premature infants. • Most congenital umbilical hernias close spontaneously by age 5 years. If closure does not occur by this time, elective surgical repair is usually advised. • Adults with small, asymptomatic umbilical hernias may be followed clinically. • Surgical treatment is offered if a hernia is observed to enlarge, is associated with symptoms, or if incarceration occurs. In the latter situation, emergent surgical treatment consisting of primary sutured repair is performed.
EPIGASTRIC ( LINEA ALBA ) HERNIA • Epigastric hernias are located in the midline between the xiphoid process and the umbilicus. • They are generally small, may be multiple, and at elective repair, are usually found to contain omentum or a portion of the falciform ligament. • It is common in middle-aged manual workers.
SPIGELIAN HERNIA ( HERNIA OF THE LINEA SEMILUNARIS ) • Spigelian hernias can occur anywhere along the length of the Spigelian line or zone—an aponeurotic band of variable width at the lateral border of the rectus abdominus. • The most frequent location of these rare hernias is at or slightly above the level of the arcuate line. • These are not always clinically evident as a bulge, and may come to medical attention because of pain or incarceration. SPIGELIAN HERNIA
SEPARATION OF THE RECTI ABDOMINIS Separation of the rectiabdominis occurs in elderly multiparous women with weak abdominal muscles . The aponeuroses forming the rectus sheath become excessively stretched. When the patient coughs or strains, the recti separate widely , and a large hernia sac ,containing abdominal viscera, bulges forward between the margins of the recti. This can be corrected by wearing a suitable abdominal belt . Surgical correction of a severe rectus diastasis by plication of the anterior rectus sheath may be undertaken for cosmetic indications, or if it is associated with disability of abdominal wall muscular function.
INCISIONAL HERNIA • Incisional hernias result from a healing failure of a prior abdominal wall surgical closure. • careful investigation shows that they occur in at least 10 to 15% of all laparotomy incisions. • Incisional hernias may be asymptomatic or present with pain, incarceration, or strangulation. • Risk factors for the development of a ventral incisional hernia include : • Postoperative wound infection. • Malnutrition. • Obesity. • Immunosuppression,. • Chronically increased intra-abdominal pressure.
INTERNAL HERNIA • Occasionally, a loop of intestine enters a peritoneal recess ( e.g., the lesser sac or the duodenal recess) and becomes strangulated at the edge of the recess. • Clinically: intestinal obstruction. • Diagnosis: by C.T Scan.
LUMBAR HERNIA The lumbar hernia occurs through the lumbar triangle and is rare. The lumbar triangle ( Petit’s triangle) is a weak area in the posterior part of the abdominal wall. It is bounded anteriorly by the posterior margin of the external oblique muscle, posteriorly by the anterior border of the latissimusdorsi muscle, and inferiorly by the iliac crest. The floor of the triangle is formed by the internal oblique muscle and the transversusabdominis muscles. The neck of the hernia is usually large, and the incidence of strangulation low.
THANK YOU Abdul.Kader WEISS 2009